0189
Thalamic Substructures in Alcoholism: Volume Deficits and Functional Correlates1Neuroscience, SRI International, Menlo Park, CA, United States, 2Stanford University, Stanford, CA, United States, 3Department of Medical Imaging, The University of Arizona Health Sciences, Tucson, AZ, United States
Synopsis
Volumes of 5 thalamic substructures—mediodorsal (MD), anterior (AV), ventral lateral posterior (VLp), ventral posterior lateral (VPl), pulvinar (Pul))—were quantified using a novel automated segmentation algorithm in 40 individuals with Alcohol Use Disorder (AUD) and 60 controls (Con). Multiple regressions on supratentorial-volume-corrected measures revealed that volumes of AV, VLp, VPl, and Pul were smaller with older age, and volumes of AV, VLp, Pul, and MD were smaller in the AUD than Con group. Functional ramifications of thalamic substructures indicated relations between back pain and smaller Pul and VLp volumes, and poor ataxia scores with smaller VPI volumes.
Introduction
The current standard of measuring global, undifferentiated brain structures is too coarse to distinguish substructural volumes, such as those of the thalamus, which may be differentially affected by Alcohol Use Disorders (AUD) and other pathologies. We used white-matter-nulled MPRAGE1 for automatic segmentation2 to investigate the effects of AUD and related pathology on thalamic substructures.Methods
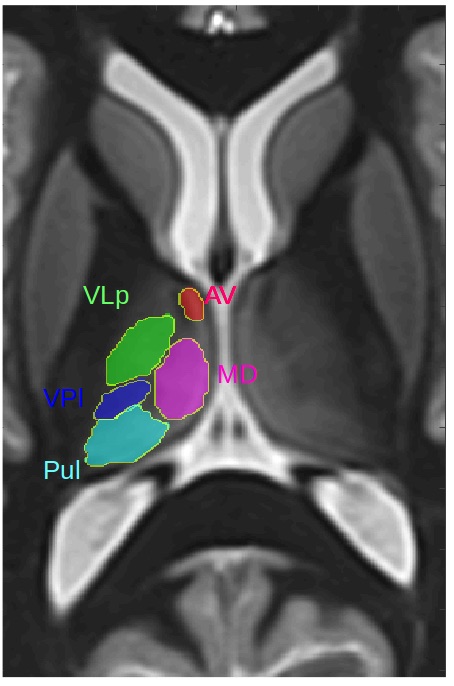
After informed consent, 60 healthy controls (aged 50.3±14.2, 29 women) and 40 adults meeting criteria for AUD (aged 53.4±8.2, 13 women)- matched on sex, age, and handedness- were scanned on a GE 3T MRI system to acquire white-matter-nulled (WMn)-MPRAGE images with 1mm isotropic spatial resolution. A multi-atlas segmentation method was used for thalamic parcellation2. The atlas comprised 20 WMn-MPRAGE datasets with manual delineations of thalamic nuclei performed by a neuroradiologist guided by the Morel atlas3 (Fig 1). Five thalamic nuclei were considered: mediodorsal (MD), anterior ventral (AV), ventral lateral posterior (VLp), ventral posterior lateral (VPl), and pulvinar (Pul).
Analysis. Each thalamic substructure volume was corrected for supratentorial brain volume (i.e.,). Multiple regressions conducted for each substructure tested 3 factors and interactions: diagnosis, age, and sex. Relevant variables were evaluated for potential correlations with each substructure.
Results
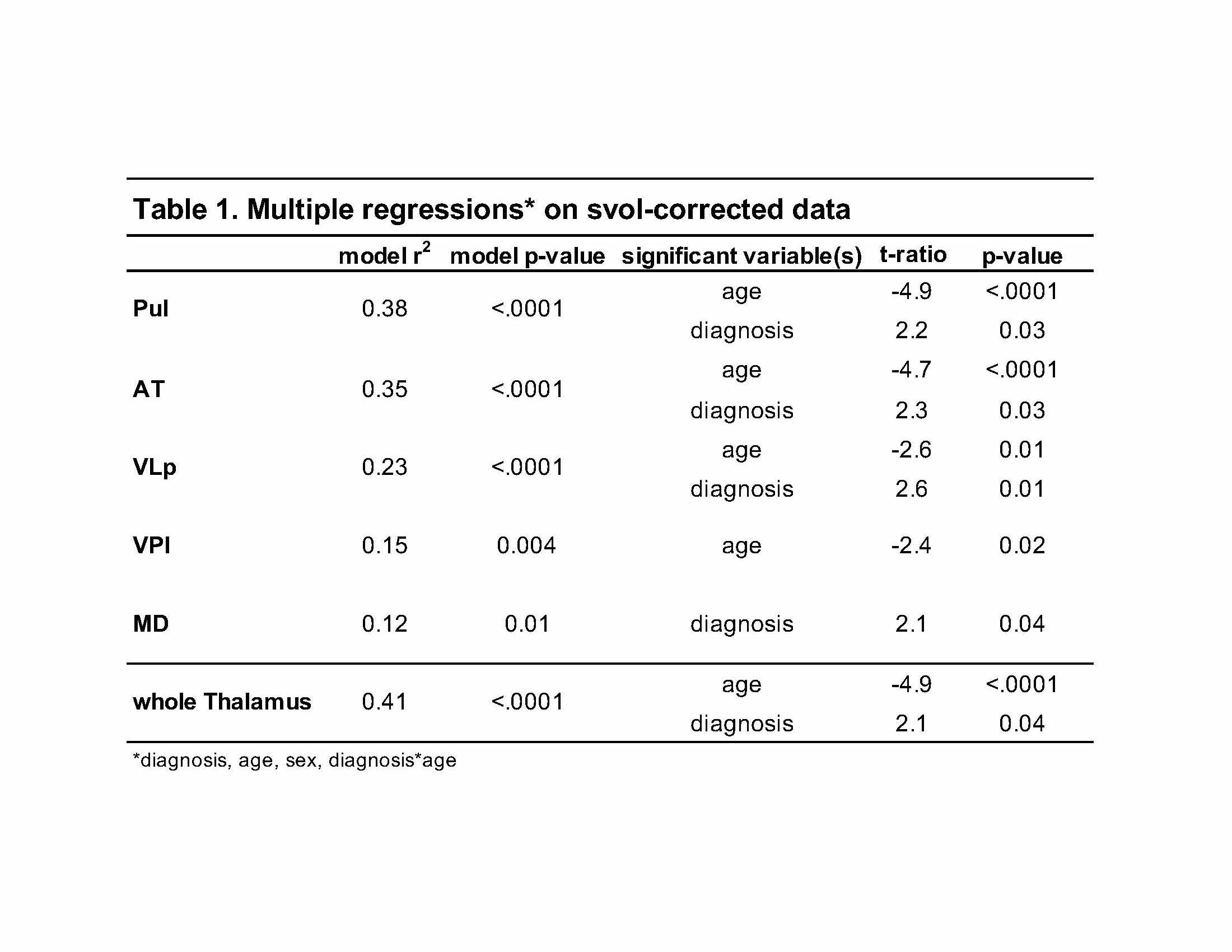
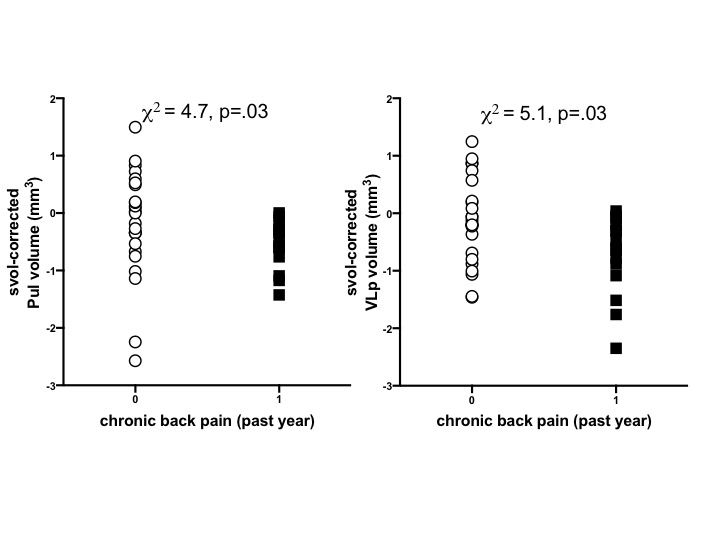
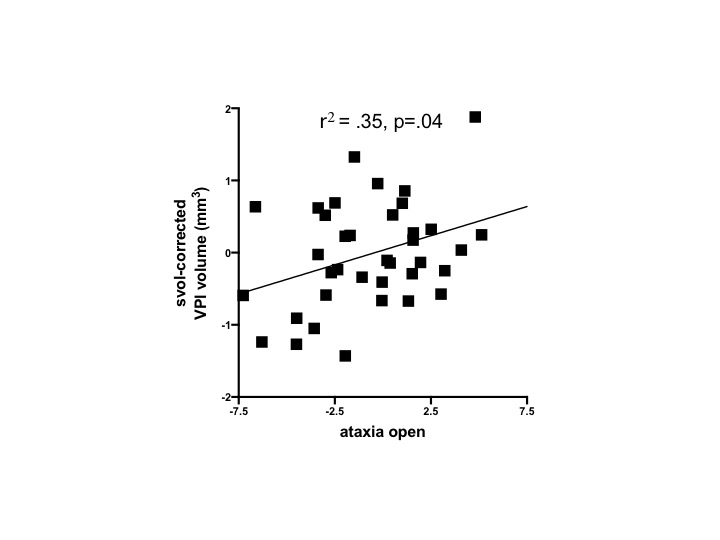
Age and diagnosis (but not their interaction) together explained 38% of the variance in Pul volume, 35% of the variance in AT, and 23% of variance in VLp. Age alone explained 15% of the variance in VPl and diagnosis alone explained 12% of the variance in MD (Table 1). For all substructures, volumes were smaller with older age and in AUD. Alcoholics relative to controls had a higher incidence of chronic back pain in the past year (p=.01) and performed worse on ataxia with eyes open (p=.03). In the AUD group only, self-report of chronic back pain was associated with smaller volumes of Pul (p=.03) and VLp (p=.03) (Fig 2). Worse performance on ataxia with eyes open was associated with smaller volume of the VPl (r2=.35, p=.04) (Fig 3).Discussion
These results confirm and extend our previous findings regarding substructures of the thalamus in AUD4. As previously reported, Pul, AV, VLp, and VPl were sensitive to age; Pul, AV, VLp, and MD were sensitive to alcoholism (cf.,5) . We extend our previous work by demonstrating, in alcoholics, selective relations between chronic back pain and smaller volumes of the Pul and VLp and between poor ataxia performance and volume of the VPl. The Pul, as a limbic structure of the thalamus, has been a target (i.e., lesion) for relief of chronic pain since the 1970’s (e.g.,6, 7). The relation between chronic back pain and VLp comports with a recent fMRI study suggesting that the magnitude of chronic pain maps to the ventral lateral thalamus8. As the VPl is a somatosensory thalamic nucleus, and receives dense input from the spinothalamic tract9, a relation with ataxia was novel, but not unexpected.Conclusion
These results demonstrate the utility of using automatic segmentation of 3T WMn- MPRAGE data to delineate the thalamic nuclei and reveal the unique liability to individual nuclei to alcoholism, pain, and motor performance.Acknowledgements
NIH Grants: R21 AA023582, R01 AA005965, U01 AA017347References
1. Saranathan M, Tourdias T, Bayram E, Ghanouni P, Rutt BK. Optimization of white-matter-nulled magnetization prepared rapid gradient echo (MP-RAGE) imaging. Magn Reson Med. 2014. 2. Thomas FT, Su J, Rutt BK, Saranathan M. A method for near realtime automated segmentation of thalamic nuclei. ISMRM, 2017, Honolulu, HI. 3. Tourdias T, Saranathan M, Levesque IR, Su J, Rutt BK. Visualization of intra-thalamic nuclei with optimized white-matter-nulled MPRAGE at 7T. NeuroImage. 2014;84:534-45. 4. Zahr NM, Saranathan MK. Substructural Volumes of the Thalamus in Alcoholism. ISMRM, 2017, Honolulu, HI. 5. Harding A, Halliday G, Caine D, Kril J. Degeneration of anterior thalamic nuclei differentiates alcoholics with amnesia. Brain. 2000;123:141-54. 6. Mayanagi Y, Bouchard G. Evaluation of stereotactic thalamotomies for pain relief with reference to pulvinar intervention. Applied Neurophysiology. 1976;39:154-7. 7. Yoshii N, Fukuda S. Effects of unilateral and bilateral invasion of thalamic pulvinar for pain relief. The Tohoku journal of experimental medicine. 1979;127:81-4. 8. Davis DA, Ghantous ME, Farmer MA, Baria AT, Apkarian AV. Identifying brain nociceptive information transmission in patients with chronic somatic pain. Pain Reports. 2016;1:e575. 9. Craig AD. Retrograde analyses of spinothalamic projections in the macaque monkey: input to ventral posterior nuclei. The Journal of Comparative Neurology. 2006;499:965-78.Figures