0181
Spiral-MRSI and tissue segmentation of normal-appearing white matter and white matter lesion load in relapsing remitting Multiple Sclerosis.1School of Health Sciences, University of Newcastle, Newcastle, Australia, 2Hunter Medical Research Institute, Newcastle, Australia, 3Department of Neurology, John Hunter Hospital, Newcastle, Australia, 4School of Medicine and Public Health, University of Newcastle, Newcastle, Australia, 5Institute of Health and Biomedical Innovation, Queensland University of Technology, Brisbane, Australia, 6Department of Radiology, Massachusetts General Hospital, Harvard Medical School, Boston, MA, United States
Synopsis
The study evaluated a novel Fast-MRSI technique with tissue segmentation in determining metabolic alterations in NAWM and WM-lesions in MS compared to healthy controls. 3D-MPRAGE and 3D-Spiral-MRSI covering 70% of total brain on 16 RRMS and 9 HCs (aged 22-55yrs) were used. MRSI was processed using MATLAB and LCModel. Findings revealed that (NAA/tCr) in WM-lesions was significantly lower than NAWM-MS and HCs. Volumetric segmentation using SIENAX, revealed a significant WBV reduction and CSF increase in RRMS compared to HCs. Fast-MRSI may enhance diagnosis and clinical monitoring of MS patients, and is sensitive in diagnosing MS even in NAWM.
Background
Multiple Sclerosis (MS) is an immune-mediated demyelinating condition, leading to neuroaxonal injury, demyelination and gliosis of the brain and spinal cord.1,2
The diagnosis and management of MS has become increasingly reliant on non-invasive MR. Conventional MRI is not adequate to understand the pathological changes of MS. Novel 1H-MRS methods might add clinical value and potentially identify new biomarkers 3,4. Additionally, it may quantify neuronal damage within both MS-lesions and normal-appearing white matter (NAWM) 5. Previous studies have used MRS to evaluate spectroscopic changes within NAWM in MS patients in comparison to healthy controls (HCs) 6,7.The challenge for these methods was to produce high resolution metabolic maps of the brain, and to measure MS-lesions and NAWM in small multi-voxels.
We designed this study to evaluate the performance of Spiral-MRSI and tissue segmentation of the whole brain, as a means of investigating metabolic changes in NAWM and white matter lesions (WML) of relapsing remitting MS (RRMS) compared to age and sex-matched HCs.
Materials and Methods
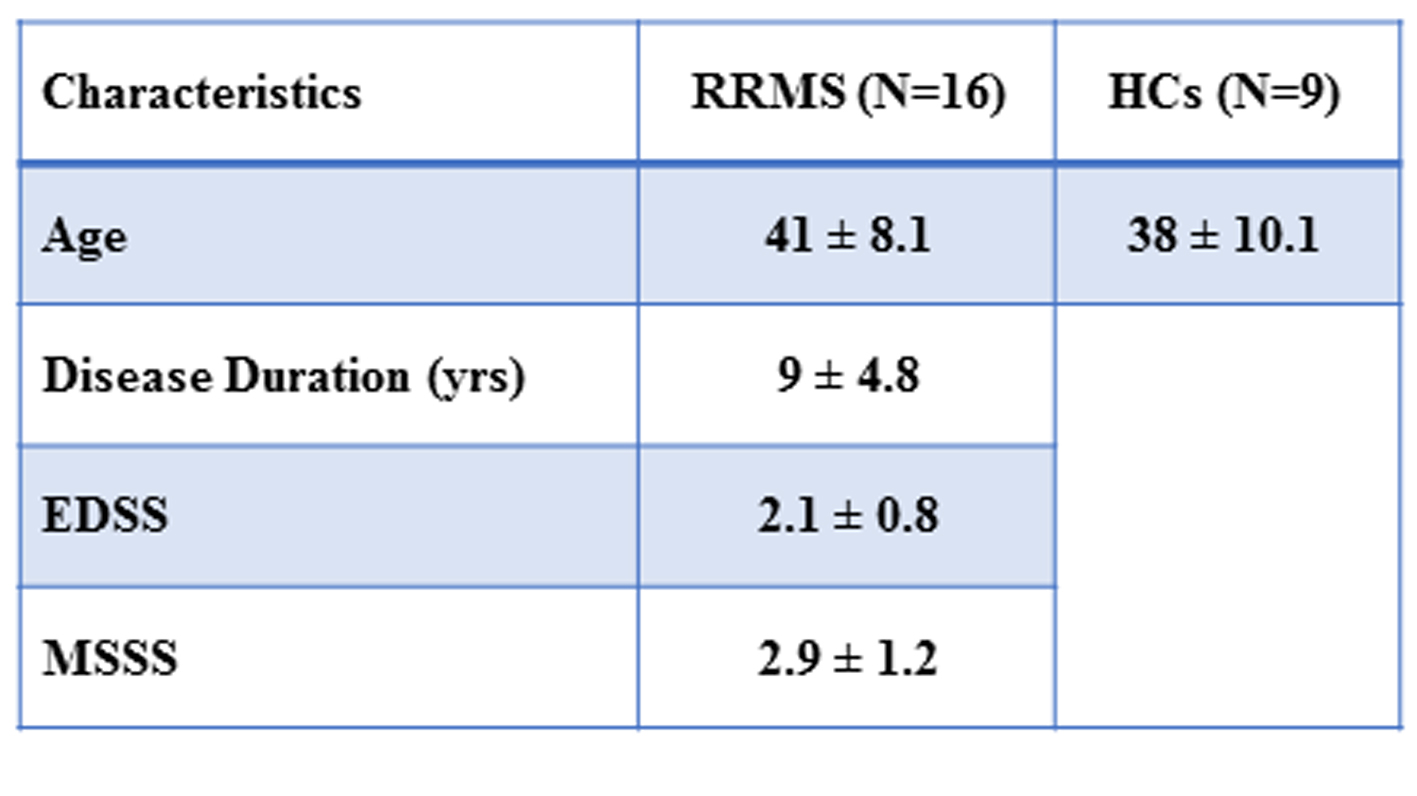
This study involved 16 MS patients, aged between 20 to 55 yrs, who had a confirmed diagnosis of RRMS according to the McDonald criteria. Nine HCs were age and sex-matched to the MS cohort.
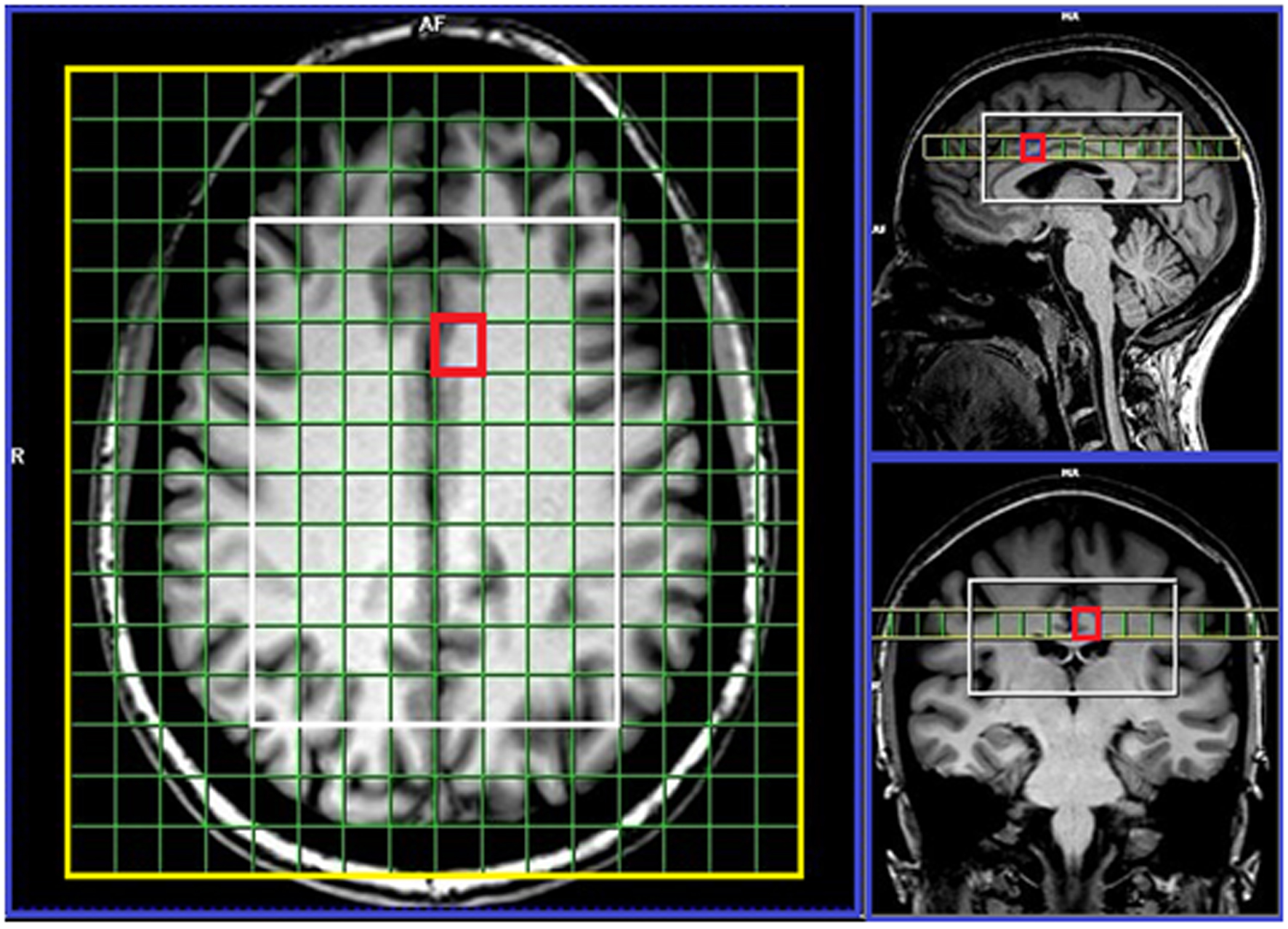
All MRI/MRS were undertaken on a 3T scanner equipped with a 64-channel coil at the Hunter Medical Research Institute, Australia. Isotropic T1-MPRAGE (TR/TE/TI=2000/3.5/1100 ms, FOV:256x256 mm, voxel size:1mm3) as well as 3D T2-FLAIR (TR/TE/TI=5000/386/1800ms, 12° flip angle, FOV=256x256 mm, voxel size:1mm3) were acquired. MPRAGE was reconstructed online into 1mm coronal and axial slices to guide voxel positioning (Fig.1). MRSI data were acquired with the following acquisition parameters: TR/TE:2800/30ms, 6 averages, spiral phase encoding, vector size:512, isotropic voxel size: 1cm3, delta frequency:3.2ppm, water suppression: On, VOI in (AP-RL-HF):10x8x4cm and acquisition time 13.38 minutes. 75% of the brain above corpus callosum was evaluated using 80 voxels.
Quantification of hyperintense WML were performed using T2-FLAIR data, while whole brain volume (WBV), cerebrospinal fluid (CSF), gray matter (GM) and white matter (WM) volumes were derived using SIENAX 8. The MRSI voxel was segmented for each voxel along one slice within the VOI, using a custom made MATLAB code and SPM12, into CSF, GM, WM and T2 lesion load. Lesions, within the MRS voxel, were segmented using the lesion growth algorithm described in our method.9
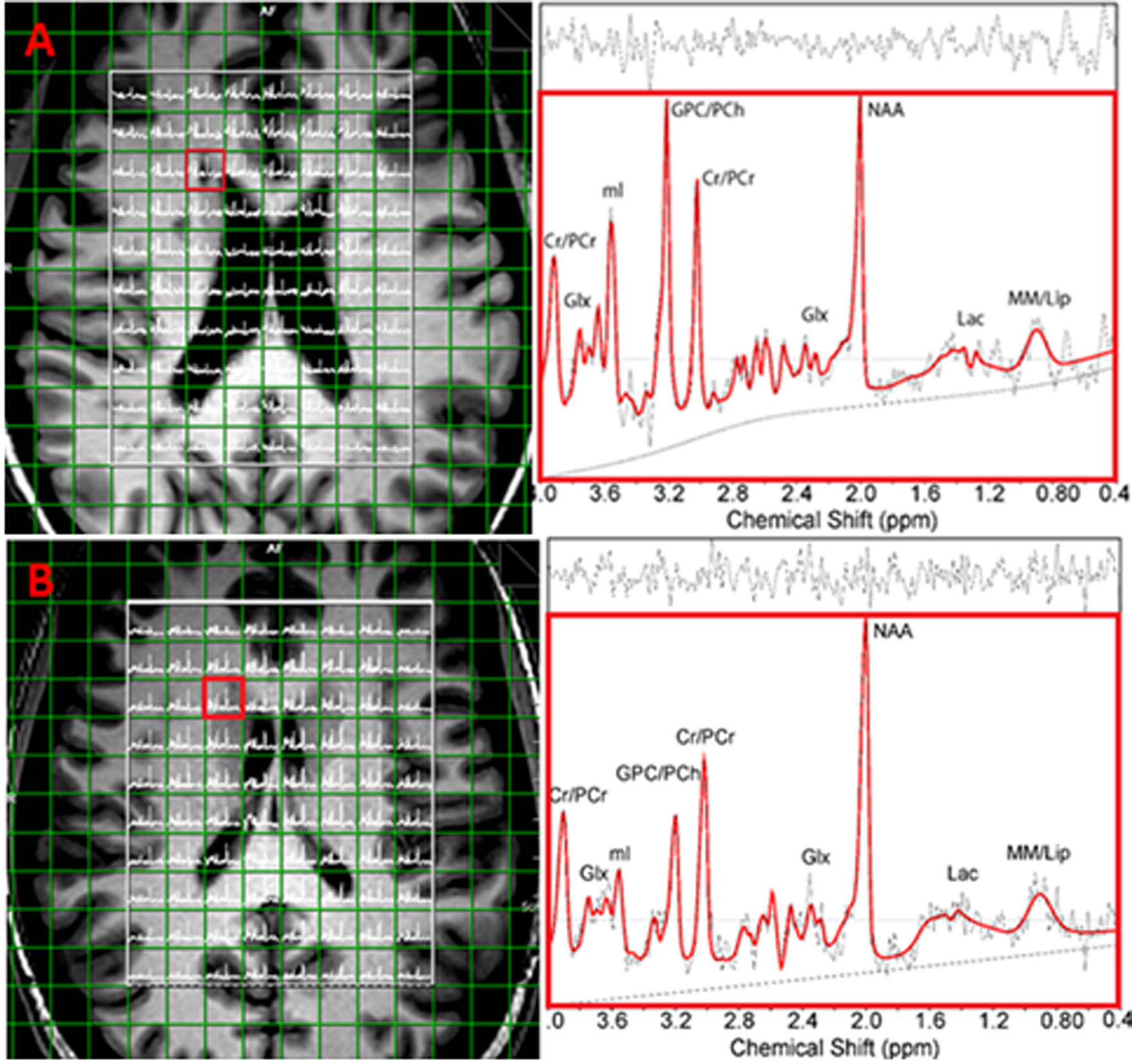
The 3D MRSI voxel was analysed using LCmodel, with a basis set matching the magnetic field and pulse sequence parameters. Spectroscopic data were reconstructed into 10×8×4 voxels with an individual voxel volume of 1cm3. Metabolic voxel data, with line width>12 Hz, CSF> 40% or Cramer Rao lower bound (CRLB(SD %))>40%, were excluded from analysis. Comparisons of mean metabolite ratios between groups for each voxel were undertaken using independent and paired-samples T-tests.
Results
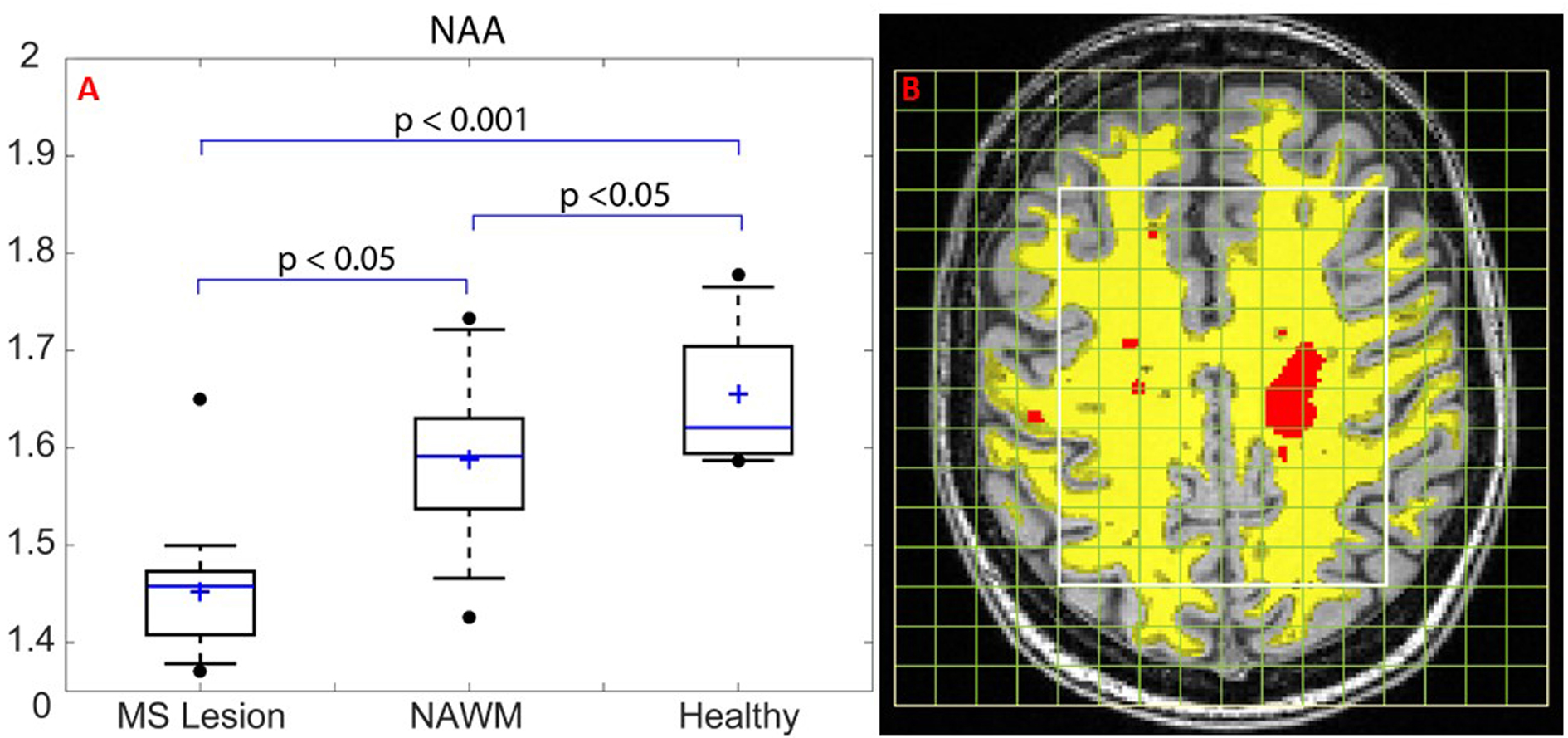
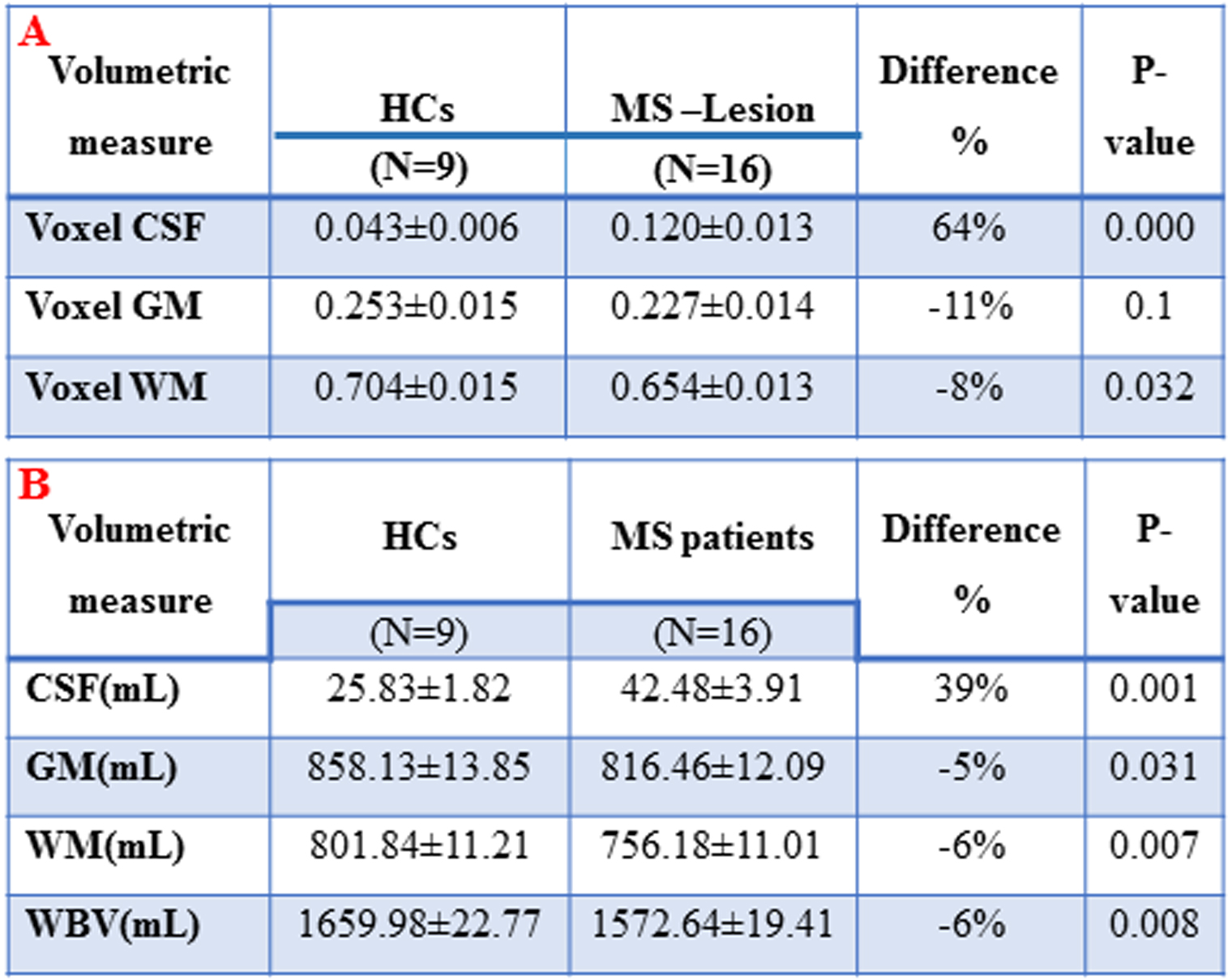
Demographic and clinical parameters of study cohorts are shown in Table 1. The performance of the Fast-MRSI technique and quantification, was applied on 15 analysed metabolites and the difference between RRMS and HCs voxels are shown in (Fig. 2). Spectroscopic voxel data within the VOI revealed that N-acetylaspartate/total creatine( NAA/tCr) in WML was significantly lower than NAWM-MS and HCs within deep cortical white matter in both posterior parietal lobes (Fig. 3A), while myo-inositol (mI) in WML(0.75±0.03) was significantly higher than NAWM-MS (0.66±0.01) and HCs (0.68±0.02). Segmentation data of WML and NAWM voxels in MS, within the VOI is shown in (Fig. 3B) and partial volume fraction within MS–lesion voxels compared to HCs summarised in Table 2A. Volumetric segmentation data indicated a significant reduction (-6%) in WBV, with a reciprocal 39% increase in CSF in RRMS compared to HCs Table 2B. On average, RRMS had a total lesion volume of 8.87mL.Discussion
The decreased NAA/tCr is in agreement with previous reports from conventional MRSI techniques10. Our findings confirmed that decreased NAA can distinguish MS from HCs not only in lesions, but also in NAWM. We also observed that mI is increased not only in NAWM11 but also in WML5 relative to HCs, indicating axonal loss, demyelination and increased glial activity. Lower WBV is associated with accelerated disease progression and reduced efficacy of therapy in MS12. MRS may be more sensitive to change in MS than WML and atrophy.Conclusions
Whole brain Fast-MRSI can be used to assess neurometabolite changes at short TE and at 3T. MRSI may enhance diagnosis and clinical monitoring of MS patients, and is a sensitive method to diagnose MS as it detects abnormality even in NAWM. Longitudinal studies are important to evaluate the effectiveness of Fast-MRSI with progression of MS.Acknowledgements
This research was supported by the Imaging Centre of the University of Newcastle and Hunter Medical Research Institute.References
1. Rovira A, Auger C, and Alonso J. Magnetic resonance monitoring of lesion evolution in multiple sclerosis. Ther Adv Neurol Disord. 2013; 6(5): 298-310.
2. Sajja BR, Wolinsky JS, and Narayana PA. Proton magnetic resonance spectroscopy in multiple sclerosis. Neuroimaging Clin N Am. 2009; 19(1): 45-58.
3. De Stefano N, Bartolozzi ML, Guidi L, et al. Magnetic resonance spectroscopy as a measure of brain damage in multiple sclerosis. J Neurol Sci. 2005; 233(1-2): 203-8.
4. Muhlert N, Atzori M, De Vita E, et al. Memory in multiple sclerosis is linked to glutamate concentration in grey matter regions. Journal of Neurology Neurosurgery and Psychiatry. 2014; 85(8): 834-840.
5. Marshall I, Thrippleton MJ, Bastin ME, et al. Characterisation of tissue-type metabolic content in secondary progressive multiple sclerosis: a magnetic resonance spectroscopic imaging study. J Neurol. 2018; 265(8): 1795-1802.
6. Brief EE, Vavasour IM, Laule C, et al. Proton MRS of large multiple sclerosis lesions reveals subtle changes in metabolite T(1) and area. NMR Biomed. 2010; 23(9): 1033-7.
7. Tiberio M, Chard DT, Altmann DR, et al. Metabolite changes in early relapsing-remitting multiple sclerosis. A two year follow-up study. J Neurol. 2006; 253(2): 224-30.
8. Smith SM, Zhang Y, Jenkinson M, et al. Accurate, robust, and automated longitudinal and cross-sectional brain change analysis. Neuroimage. 2002; 17(1): 479-89.
9. Quadrelli S, Mountford C, and Ramadan S. Hitchhiker's Guide to Voxel Segmentation for Partial Volume Correction of In Vivo Magnetic Resonance Spectroscopy. Magnetic Resonance Insights. 2016; 9(1-8.
10. Rahimian N, Saligheh Rad H, Firouznia K, et al. Magnetic resonance spectroscopic findings of chronic lesions in two subtypes of multiple sclerosis: primary progressive versus relapsing remitting. Iran J Radiol. 2013; 10(3): 128-32.
11. Aboul-Enein F, Krssak M, Hoftberger R, et al. Reduced NAA-levels in the NAWM of patients with MS is a feature of progression. A study with quantitative magnetic resonance spectroscopy at 3 Tesla. PLoS One. 2010; 5(7): e11625.
12. Sormani MP, Kappos L, Radue EW, et al. Defining brain volume cutoffs to identify clinically relevant atrophy in RRMS. Mult Scler. 2017; 23(5): 656-664.
Figures