0177
Remote metabolic profile changes in subacute spinal cord injury1Department of Radiology, Swiss Paraplegic Centre, Nottwil, Switzerland, 2Institute for Biomedical Engineering, ETH and University of Zurich, Zurich, Switzerland, 3Max-Planck Institute for Biological Cybernetics, Tuebingen, Germany
Synopsis
Not a single MR marker has been identified to predict patient outcome in spinal cord injury (SCI) rehabilitation. Therefore, we applied magnetic resonance spectroscopy (MRS) to examine metabolite concentration in the pons around 10 weeks after injury and identify group differences in complete and incomplete SCI at the time of the MRS acquisition.
Introduction
Spinal cord injury (SCI) affects the patients in several aspects. The level and the severity of injury determines remaining function and possible recovery. Early detection of metabolic alterations along the corticospinal tract between the injury site and the brain is possible using magnetic resonance spectroscopy (MRS). MRS provides complementary biochemical information that helps to characterize the neural tissue status non-invasively. In this study, we thus measured metabolite concentrations in the brainstem of subacute SCI patients 10 weeks after injury for the first time, and we explore the results for group differences between both complete and incomplete SCI and paraplegic and tetraplegic patients.Methods
MRI Protocol & Post-Processing
20
SCI patients (age median and range: 50, 23-64 years; female: 2) participated in
this study with an MRS measurement at around 10 weeks (median: 71.5 days,
range: 37-84) after acute injury. 17 healthy volunteers (age median and range: 52,
31-68 years; female: 2) served as a control group. The measurements were performed
on a 3T scanner (Achieva, Philips Healthcare, Best, The Netherlands) using a
SENSE head coil. A 3D T1 weighted MRI sequence (1x1x1mm3) and a
spectroscopic scan (PRESS localization, TE=30ms, TR=1600ms) were applied. The
spectroscopic voxel (25x20x20 mm3) was placed in the pons. All MRS
measurements contained 128 signal averages and were fitted with LCModel (Provencher,
1993) using 18 metabolites in the basis set. The metabolites were quantified
individually and the internal water concentration served as reference standard1.
Clinical Assessment
The clinical status of
the patients was assessed according to the International Standards for
Neurological Classification of Spinal Cord Injury (ISNCSCI) protocol for motor,
light-touch and pin-prick scores as described by Kirshblum et al2. One
of the measures specifies the severity (completeness) of the injury and was
used to stratify the patient group into incomplete (iSCI) and complete injury
patients (cSCI). The latter ones having no sensory or motor function preserved
in the sacral segments S4-S5. The level of injury specifies whether the
patients are classified as tetraplegic (tSCI, above the first thoracic spinal
disc level, Th1) or paraplegic (pSCI, site of injury at or below Th1).
Statistics
The statistical analyses
were performed with R (R Core Team, 2016, Version 3.5.0). Group differences
were assessed using the non-parametrical Kruskal-Wallis test. Post-hoc
Wilcoxon-test was used to investigate the subgroup differences.
Results
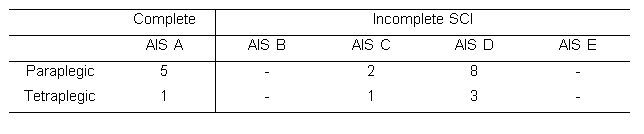
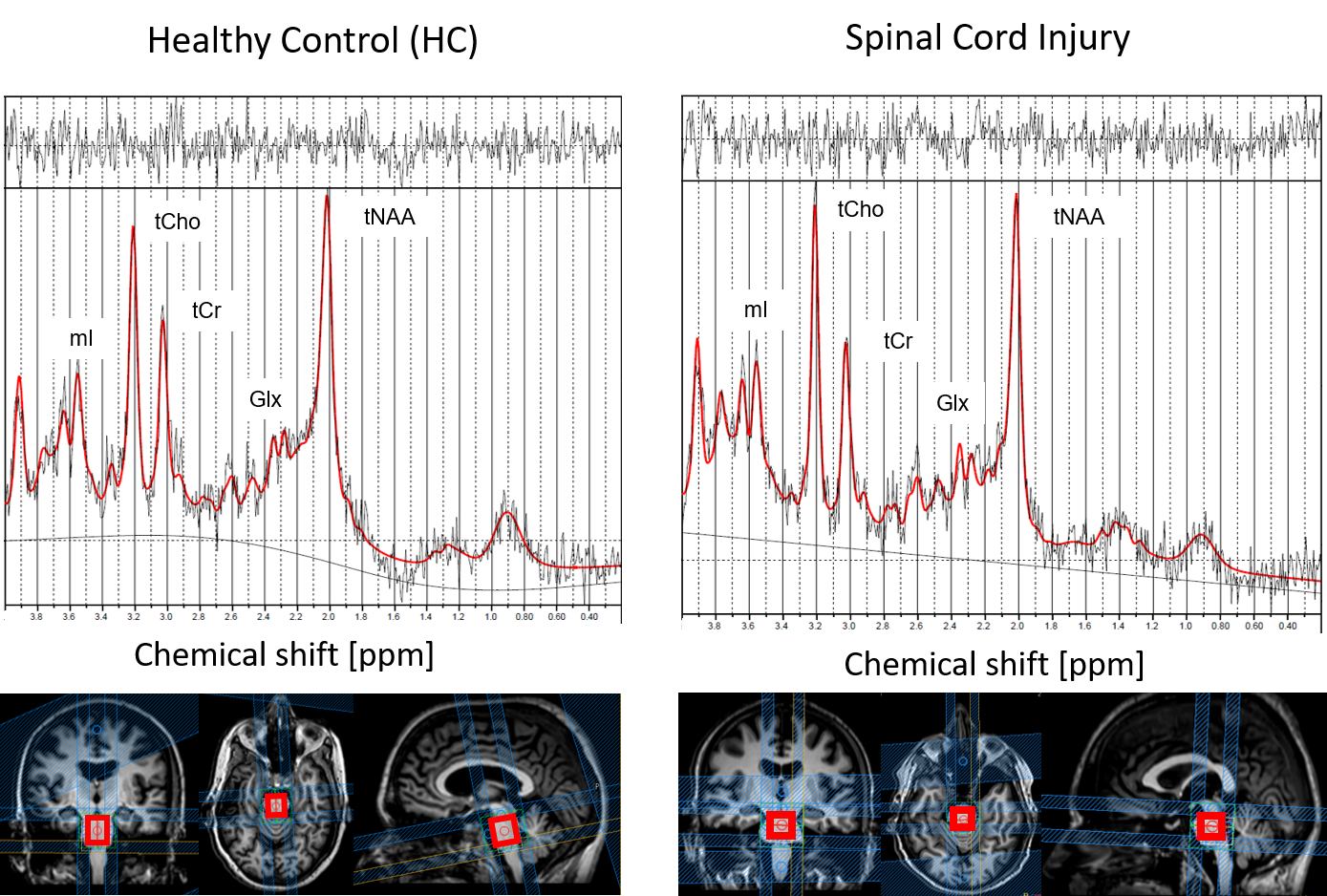
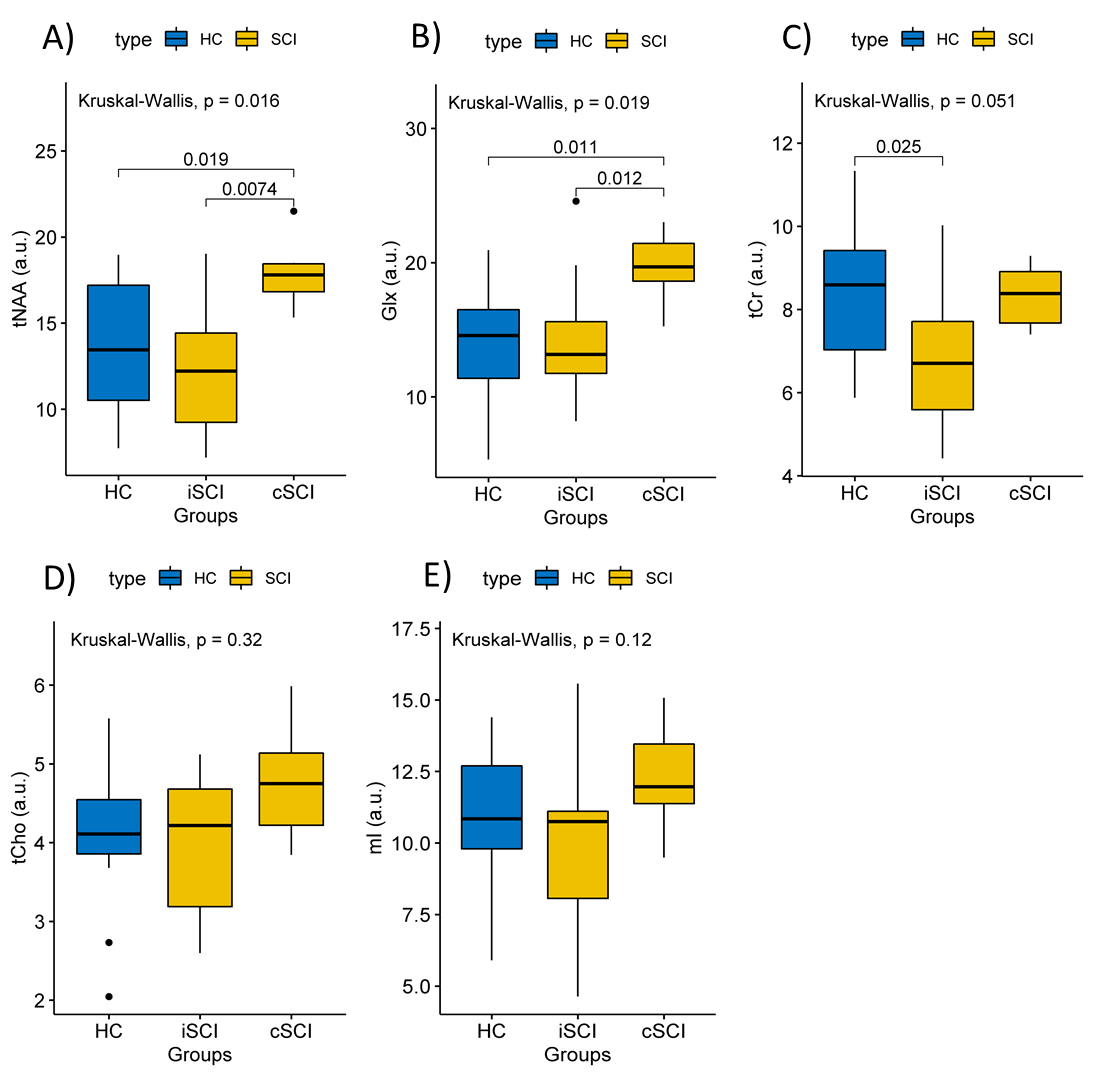
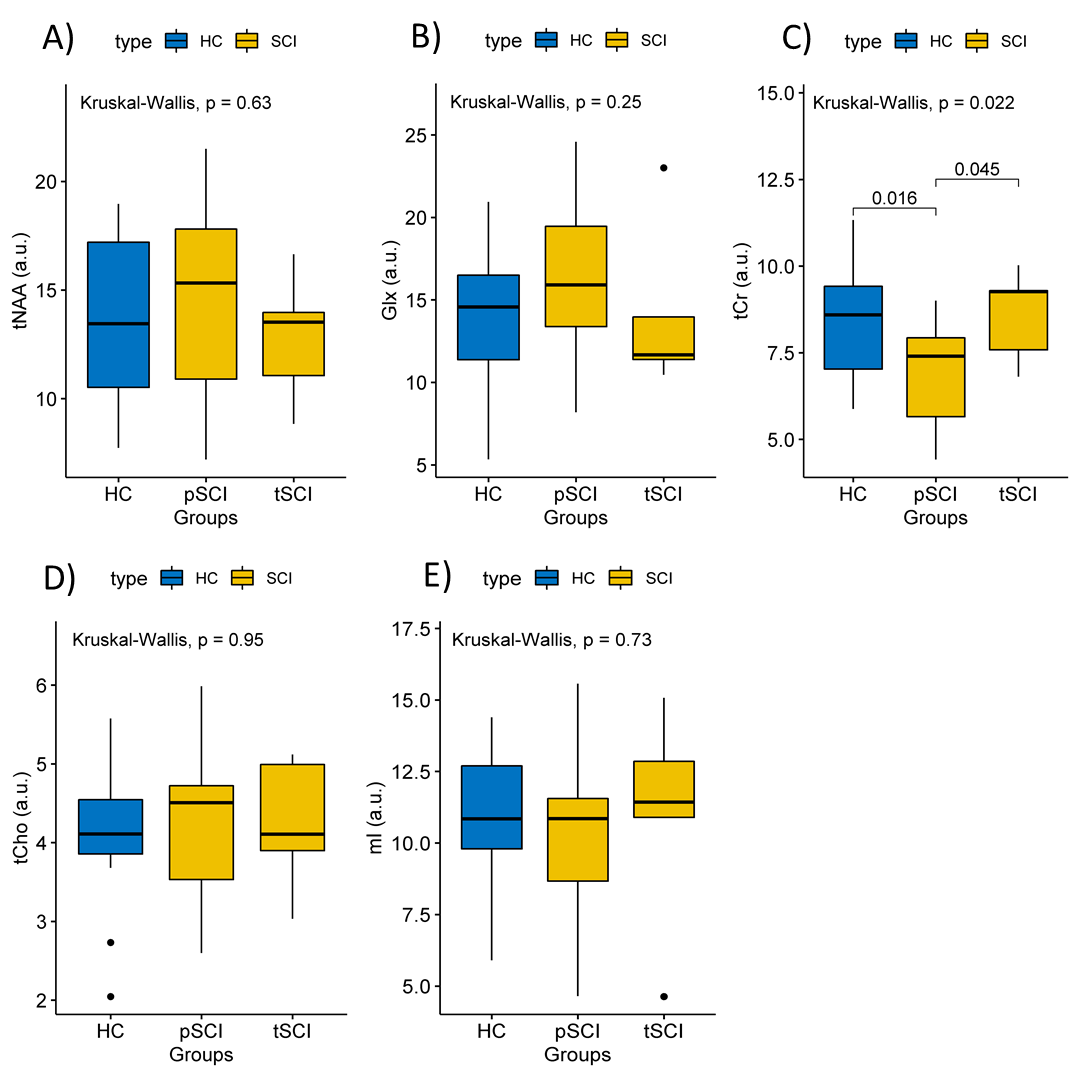
15 paraplegic and five tetraplegic SCI patients were included. 14 patients were classified as incomplete SCI and six patients as complete SCI (Fig.1). Planning site and representative spectra are shown in Fig.2. Total N-Acetyl-Aspartate (tNAA), choline containing compound (tCho), total creatine (tCr), glutamate and glutamine (Glx), and myo-Inositol (mI) were reliably detected (CRLB<25%). Group differences were found for the metabolites tNAA (P=0.016) and Glx (P=0.019). No significant differences were detected for tCr (P=0.051), tCho (P=0.32) and mI (P=0.12). Subgroup analysis showed that tNAA and Glx concentrations were higher in complete SCI compared to both healthy controls (P=0.019 and P=0.011, resp.) and incomplete SCI (P=0.0074 and P=0.012, resp.) (Fig.3). tCr was lower in paraplegic patients compared to tetraplegic patients (P=0.045) and healthy volunteers (P=0.016) (Fig.4).Discussion
We acquired spectroscopic data in 20 SCI patients around 10 weeks after injury. Spectra were acquired from the pons, which bridges the signal transfer between the different regions of the central nervous system. The main finding of this study is that two metabolic markers (tNAA and Glx) show group differences and have highest concentrations in the pons of subacute complete spinal cord injury patients, in whom no motor or sensory function is preserved below the level of injury. Previous studies show decreased tNAA in the spinal cord of chronic SCI3 and atrophy in the brainstem of chronic SCI4. tNAA is involved in myelination processes acting as acetyl donor and Glx includes the main excitatory neurotransmitter glutamate indicating a difference in neurotransmission.
In addition, tCr concentrations were lower in the pons of subacute paraplegic patients compared to tetraplegic patients and healthy controls. A lower tCr in paraplegic patients 10 weeks after the injury indicates an alteration of the energy metabolism in the pons.
Conclusion
This study shows group differences between complete versus incomplete as well as paraplegic versus tetraplegic SCI patients and HC in the pons for tNAA, Glx and tCr concentrations. Future studies should improve our understanding of the physiological basis of ongoing metabolic profile changes in the subacute phase after the acute injury.Acknowledgements
The authors thank all the patients participating in this study. Funding by the Swiss National Science Foundation (Grant Number: 143715), the University of Zurich (Clinical Research Priority Program Multiple Sclerosis), the European Union (ERC Starting Grant, SYNAPLAST MR, Grant Number: 679927) and the Swiss Paraplegic Foundation are gratefully acknowledged.References
[1]
Gasparovic C et al. Magn Reson Med 2006; 55(6): 1219-1226.
[2]
Kirshblum SC et al. Journal of Spinal Cord Medicine. 2011;34(6):535-546.
[3] Wyss PO et al. Proc Intl Soc Magn Reson Med. Paris,
France 2018: 881.
[4] Grabher P et al. NeuoImage: Clinical 2017;15:494-501.
Figures