0141
Imaging of calf muscle contraction in pediatric patients with cerebral palsy and healthy children by dynamic phase contrast MRIClaudia Weidensteiner1,2, Xeni Deligianni1,2, Francesco Santini1,2, Tanja Haas1, Philipp Madoerin1, Oliver Bieri1,2, Katrin Bracht-Schweizer3, Erich Rutz4, Meritxell Garcia5, and Reinald Brunner4
1Department of Radiology, Division of Radiological Physics, University of Basel Hospital, Basel, Switzerland, 2Department of Biomedical Engineering, University of Basel, Basel, Switzerland, 3Laboratory for Movement Analysis, University Children's Hospital Basel, Basel, Switzerland, 4Department of Orthopedic Surgery, University Children's Hospital Basel, Basel, Switzerland, 5Department of Radiology, Division of Neuroadiological Physics, University of Basel Hospital, Basel, Switzerland
Synopsis
Aim of this study is to investigate the feasibility of phase contrast imaging for assessment of muscle function in children with cerebral palsy (CP). Time-resolved cine phase contrast MRI was synchronized with electrical muscle stimulation of the calf muscle at a clinical 3T MRI scanner. 11 healthy and 4 children with hemiparetic CP were scanned. Dynamic velocity, strain, and strain rate maps were reconstructed. Synchronous dynamic PC MRI of electrically stimulated muscle is feasible in children, even in CP patients and might provide further insight into the health status of their muscles.
Introduction
Cerebral palsy (CP) is a sensorimotor dysfunction caused by damage to the not yet developed brain. This leads to weakness and spasticity of the affected muscles (1). Time-resolved phase contrast (PC) MRI can be used to study muscle function and was applied to assess voluntary leg muscle contraction in adults, e.g. in (2,3). Children with CP cannot always freely control movement of their limbs, therefore voluntary exercise paradigms are often not adequate for diagnosis and examination. A cine PC MRI method to measure involuntary muscle contraction induced by electrical muscle stimulation (EMS) has been recently developed (4), however this MRI technique was never applied to children. Aim of this study is to check the feasibility of cine PC MRI of evoked muscle contraction in pediatric patients with spastic CP.Methods
Two groups of children were included in the study: to date, 11 healthy controls (5 males, age range 9 to 16 years) and 4 CP patients with hemiparesis (3 male, age 11-12 years) were scanned. For the experimental setup, a two-channel commercially-available EMS device was used to induce involuntary periodic muscle contraction of the triceps surae muscle group of the dominant leg (in the controls) or of the most affected leg (in the patients) through self-adhesive electrodes attached to the muscle belly. The evoked force was recorded with a foot pedal device with a built-in force sensor during the scan (5). The maximum voluntary force (MVF) (without EMS) was also measured. Cine PC MRI was performed at 3T whole body clinical MRI scanner. A three-directional cine gradient echo PC velocity encoding sequence was applied with the following parameters: 3 parasagittal slices, spatial resolution 2.2x2.2x5.0 mm3, velocity encoding (VENC) 25 cm/s, temporal resolution 126 ms, TE=7.2 ms, bandwidth = 400 Hz/pixel, FOV= 280x140 mm2, 3 k-space lines per segment, acquisition time 3 min, 27 temporal phases. The MRI acquisition was synchronized to the EMS cycle (1 s ramp up, 1 s plateau, 1 s ramp down, 1 s recovery). The stimulus consisted of 30 pulses/s (pulse width 300 µs). The amplitude of the stimulation current was in the range of 15 – 28 mA and was individually adjusted for each child within its comfort levels to a point that induced visible force output of at least 5% MVF if possible. To visualize the contraction of the muscle, a ROI was manually drawn on the calf muscles and the velocity vector field was displayed for every temporal phase (4). The contraction speed was calculated for each phase as median of the magnitude of the velocity vectors in the ROI. Strain rate and strain vectors were extracted from the velocity and displacement fields. Maps of the principal strain and strain rate were displayed.Results
The maximum tolerated stimulation current and the developed force at this current showed a relatively large variability within both groups. In patients, the range of the average evoked force was 2 N – 53 N (2 – 21 % MVF). Consequently, in some children the data quality of the velocity fields was not sufficient for analysis of velocity and strain/strain rate. Data quality was sufficient in healthy children if developed force was at least 5% of the MVF. The time course of the contraction speed showed two distinctive peaks for the moments of contraction and release in 8 of the 11 healthy children and in 2 of the 4 patients. The peak contraction speeds were below 1 cm/s. Strain and strain rate maps showed activation in the whole ROI with higher localized activation in some children.Discussion
In general, the EMS was well tolerated in both groups. Even the stiff legs of the CP patients could be stimulated to develop a periodic force over 3 min. The variability of the results can be attributed to the heterogeneity of our children population (age, physical development, compliance), to the different grades of paresis in patients, and to a lower tolerance of children for EMS, which prevented the use of higher currents. Therefore, the protocol needs to be further optimized for this population, for example by reducing the VENC and thus increasing the sensitivity to low velocities. Nevertheless, the extraction of quantitative parameters related to the muscle biomechanics was already feasible and they can provide useful insight in the assessment of this disease.Conclusion
This study showed that synchronous dynamic PC MRI is feasible in electrically stimulated muscle in children, even in CP patients. This functional assessment may detect single muscles or muscle groups to be major factors for a given motor dysfunction. Work is in progress to compare the findings with physical/clinical data.Acknowledgements
The study was supported by the Swiss National Science Foundation (Grant Number 173292).References
- Mathewson MA, Lieber RL. Pathophysiology of muscle contractures in cerebral palsy. J Orthop Res. 2015 Jan;33(1):33-9.
- Mazzoli V, Gottwald LM, Peper ES, Froeling M, Coolen BF, Verdonschot N, Sprengers AM, van Ooij P, Strijkers GJ, Nederveen AJ. Accelerated 4D phase contrast MRI in skeletal muscle contraction. Magn Reson Med. 2018 Nov;80(5):1799-1811.
- Sinha U, Malis V, Csapo R, Narici M, Sinha S. Shear strain rate from phase contrast velocity encoded MRI: Application to study effects of aging in the medial gastrocnemius muscle. J Magn Reson Imaging. J Magn Reson Imaging. 2018 Nov;48(5):1351-1357.
- Deligianni X, Pansini M, Garcia M, Hirschmann A, Schmidt-Trucksäss A, Bieri O, Santini F. Synchronous MRI of muscle motion induced by electrical stimulation. Magn Reson Med. 2017 Feb;77(2):664-672.
- Santini F, Bieri O, Deligianni X, OpenForce MR: A low-cost open-source MR-compatible force sensor, Proc ISMRM 2018, #5131.
Figures
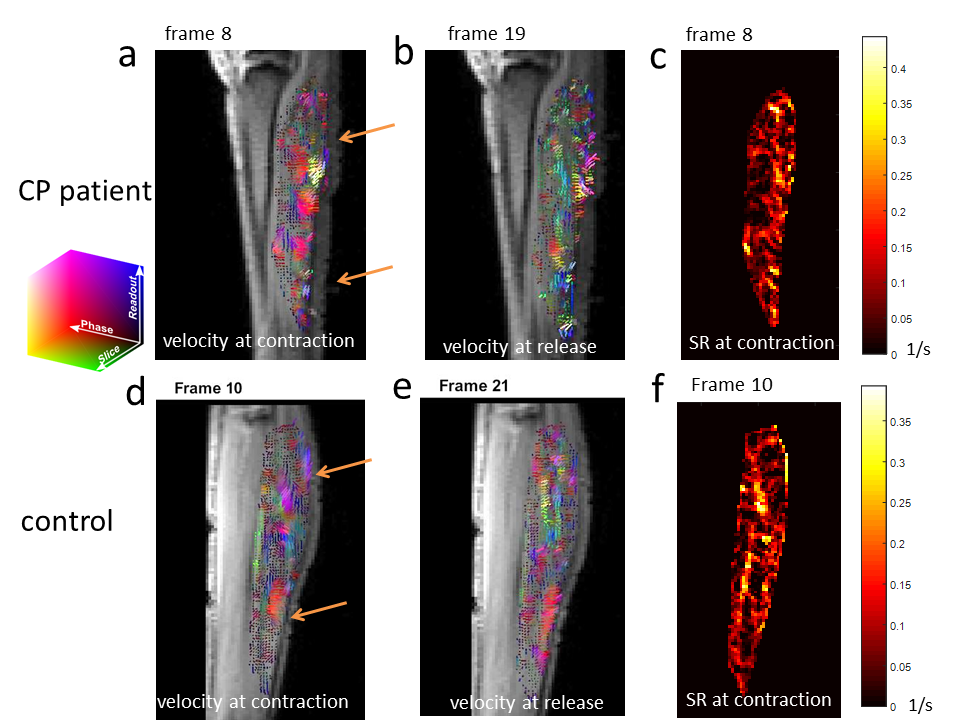
Results in
a boy with CP and paresis of the left leg (11 y, 138 cm, 36 kg) (top row) and in
a healthy girl (9 y, 137 cm, 29 kg) (bottom row) a,d) Map of the velocity
vectors in the calf muscle (color-coded for direction) at the moment of
contraction. The position of the electrodes is marked with arrows. b,e) Map of
the velocity vectors (color-coded for direction) at the moment of release. c,f)
Strain rate map at the moment of contraction. The stimulation in the patient is
more superficial than in the control.
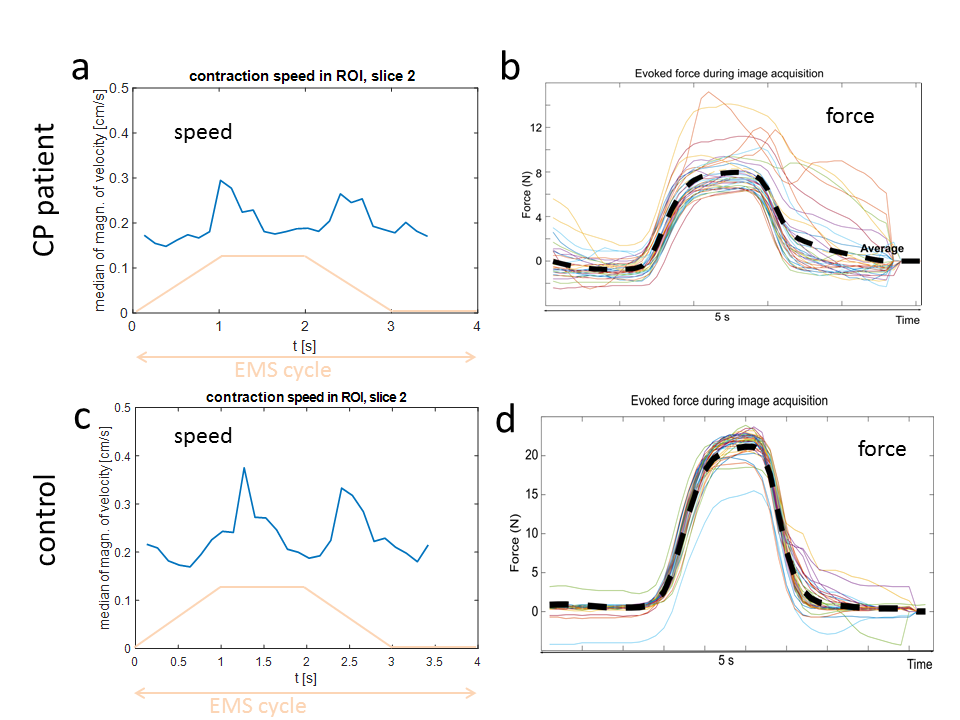
Results in
the same patient (top row) and control (bottom row) as in Fig 1 a,c) Median magnitude of velocity in
the ROI showing the peaks at the moment of contraction and release. The
waveform of the EMS is shown in orange. b,d) Time courses of force for all EMS
cycles. The average force is shown as a dashed line. The shape of the average
force is similar in patient and control, but the force time courses in the
patient have a higher variability.