0131
Five-minute single sequence comprehensive 4D pediatric ankle MRI with T2 Shuffling1Electrical Engineering and Computer Sciences, University of California, Berkeley, Berkeley, CA, United States, 2Radiology, Stanford University, Stanford, CA, United States
Synopsis
The use of volumetric acquisitions for musculoskeletal MR in clinical settings has been limited due to blurring artifacts from T2 decay. T2 Shuffling (T2Sh), a redesigned 3D fast spin-echo technique that mitigates blurring, has been successfully applied to pediatric knee MRI in a clinical setting and used to streamline the pediatric knee exam. This work assesses a shortened T2Sh scan for pediatric ankle MRI with total scan time under 5 minutes. Our results show that T2Sh has the potential to provide a comprehensive diagnostic protocol in place of the conventional long 2D exam.
Introduction
Two-dimensional (2D) fast spin-echo (FSE) is the predominant MRI method for evaluating joints due to its high resolution and flexible image contrast$$$^{1-3}$$$. Volumetric variants of FSE combined with multi-planar reformats could streamline the exams compared to scanning at multiple imaging planes$$$^{2-4}$$$. However, 3D FSE has seen limited clinical adoption due to the difficult tradeoff between scan time and image blurring$$${4,5}$$$. A 3D, multi-contrast FSE technique termed T2 Shuffling (T2Sh)$$$^6$$$ was previously described and evaluated against a conventional pediatric knee MRI protocol, indicating that missing clinically relevant pathology is unlikely when used in place of 2D FSE$$$^4$$$. Here we further develop and clinically evaluate a five-minute T2Sh scan designed for pediatric ankle MRI that reduces the image blurring without increasing scan time. We compare its image quality and imaging time to that of a conventional 2D ankle MRI protocol.Materials and Methods
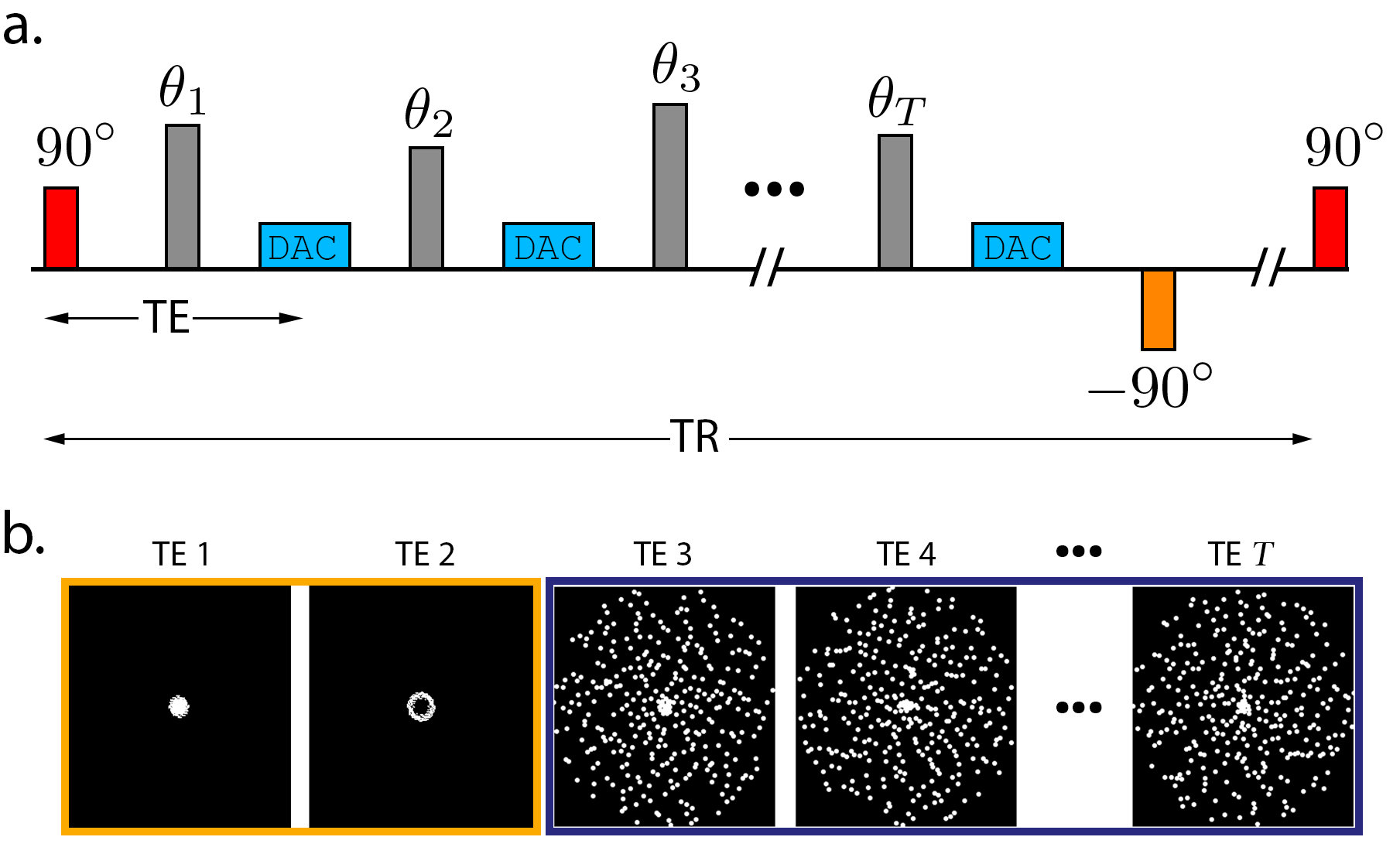
T2Sh was previously implemented to randomly re-sample k-space positions at multiple echo times, effectively supporting a four-dimensional reconstruction with volumetric images varying from proton-density (PD) to heavy T2 weighting$$$^6$$$ (Figure 1). To reduce scan time, the repetition time (TR) was reduced to 600 ms, as the increased T1 weighting was found to be tolerable due to the fast recovery module placed at the end of the FSE train. With Institutional Review Board approval, 17 consecutive children referred for ankle MRI prospectively underwent a standard clinical ankle protocol followed by T2Sh at 3T (GE MR750). Typical T2Sh scan parameters were TR/TE=600/6 ms, ETL=33, 12-channel flexible coil array, 0.6 mm isotropic resolution, fat suppression, and coronal source images. One subject was scanned with T2Sh twice to compare a longer TR/scan time. Images were reconstructed at effective echo times of 20 ms (PD-weighted) and 90 ms (T2-weighted).
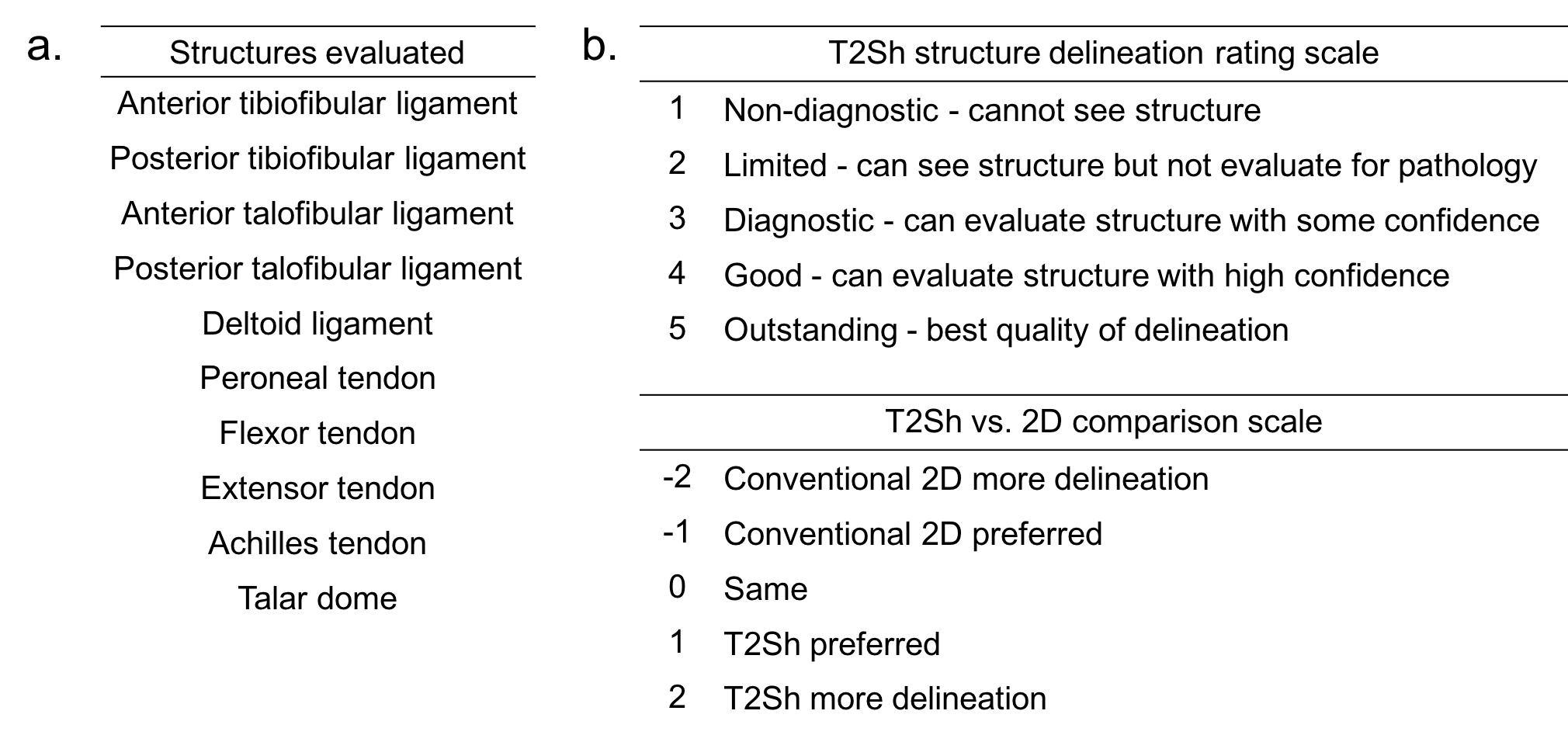
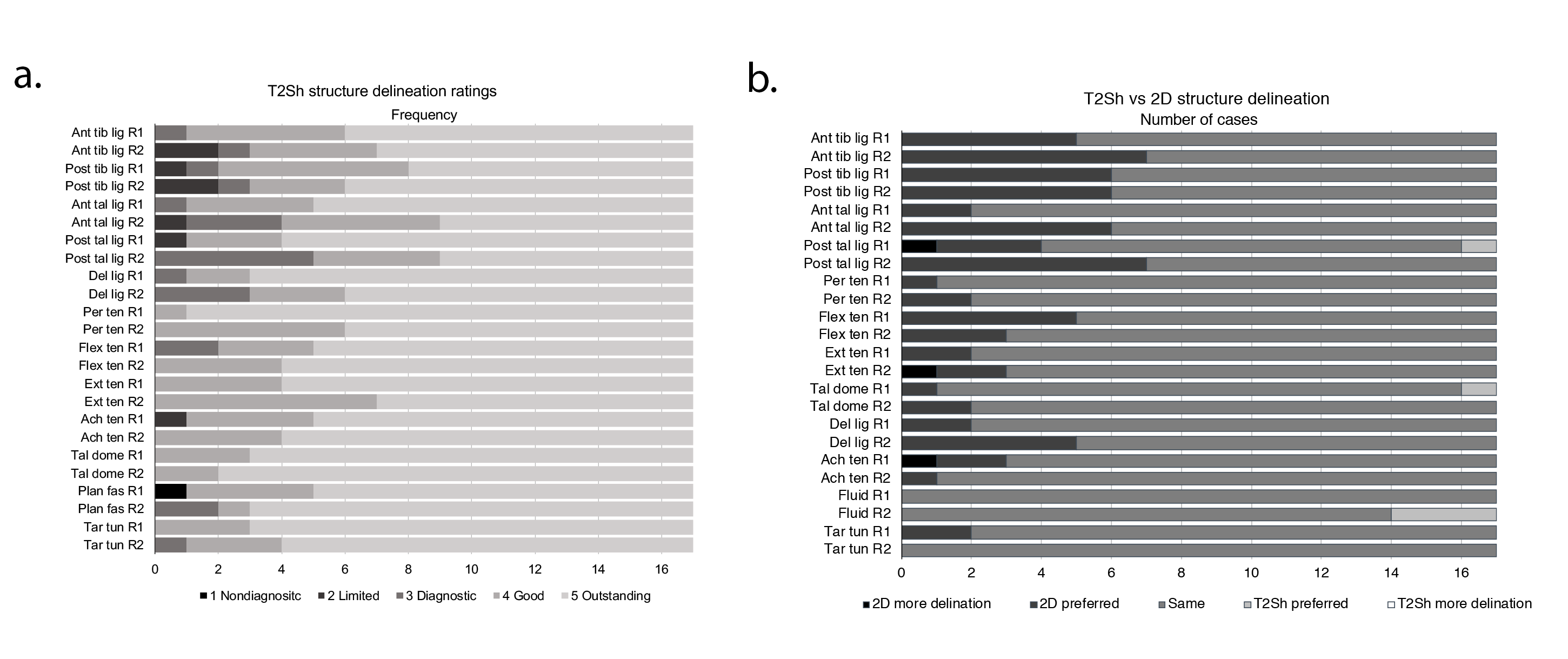
T2Sh performance was assessed by two readers blinded to diagnostic reports using a multi-planar reformat capable workstation (Osirix), and 12 anatomic structures were graded on a scale of 1 (cannot see structure) to 5 (best quality of delineation), shown in Figure 2. Relative quality of anatomic structure delineation of T2Sh and 2D sequences were also compared. A Wilcoxon signed rank-sum test assessed the null hypothesis that T2Sh structure delineation compared to conventional 2D is unchanged. Intra-class correlation coefficients were calculated for inter-observer agreement.
Results
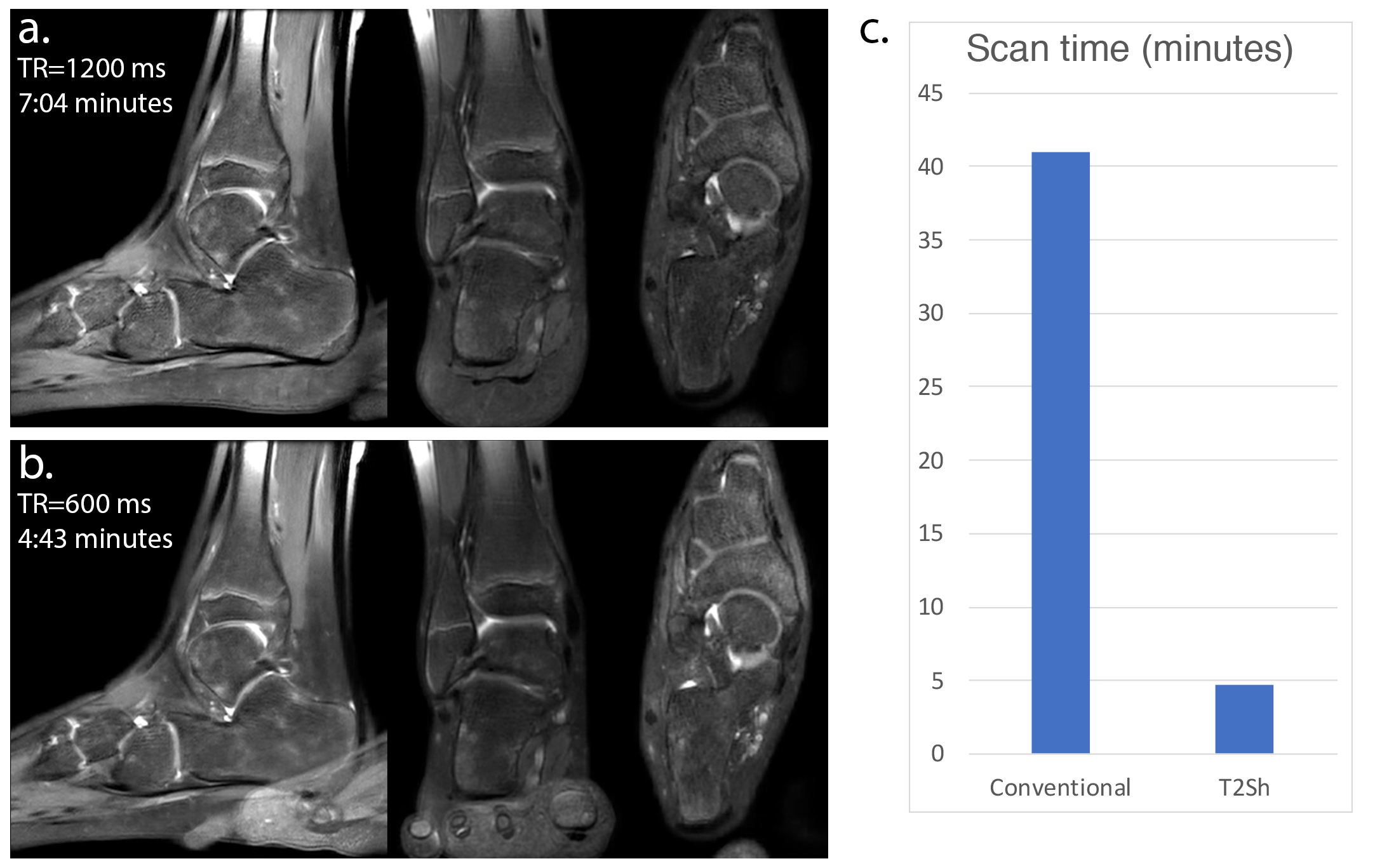
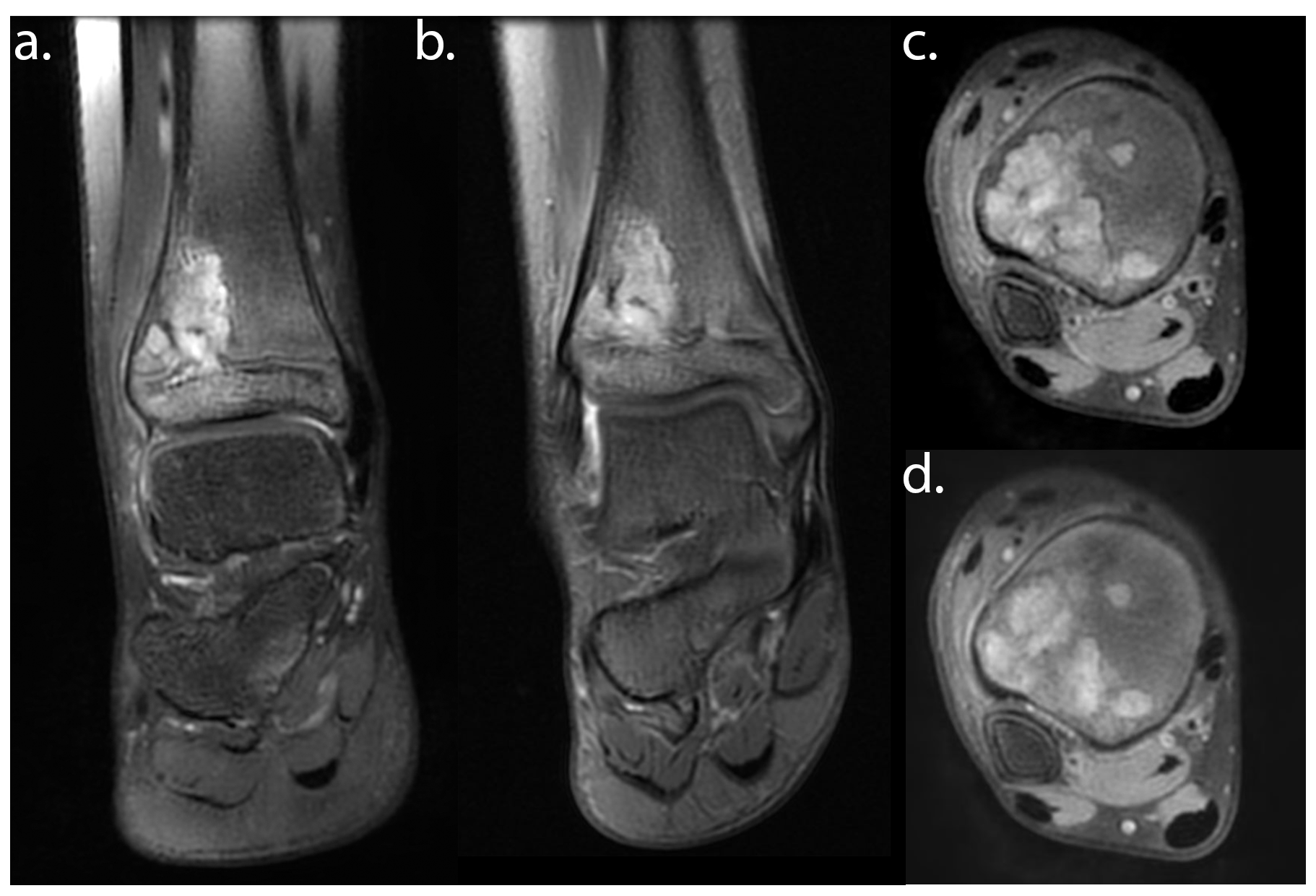
Figure 3 compares T2Sh with TR=1200 ms and 7:04 minutes scan time to T2Sh with TR=600 ms and 4:43 minutes scan time on one subject. Neglecting image wrap due to error in prescribing non-selective excitation, relative image quality and contrast is similar. Figure 4 shows representative images of T2Sh vs. 2D for an eight-year-old female with history of recurrent osteomyelitis, and highlights sharp reformats, with good delineation of short-T2 tendons.
Figure 5 summarizes the image quality ratings and comparisons between T2Sh and 2D FSE. Delineation of the 12 anatomic structures on all subjects were at least diagnostic except for one subject due to motion artifacts and one subject due to reconstruction artifacts from over-regularization. The plantar fascia delineation was limited in one additional case due to image wrap from technologist error in prescribing selective excitation. The confidence interval (CI) of diagnostic rating or better was 87%-100% (99% CI) or higher, except for the anterior/posterior tibiofibular ligaments (82%-94%). Interobserver agreement was poor to fair except for anterior/posterior ligaments, posterior talofibular ligament, deltoid ligament, and plantar fascia. There was no significant difference between T2Sh and conventional 2D structure delineation (P<.01). Typical imaging time for T2Sh and conventional exam was 4.7 and 41.0 minutes, respectively (Figure 3c).
Discussion
The proposed protocol simultaneously acquired fat-suppressed PD-weighted and T2-weighted images with 3D isotropic resolution in under five minutes. However, it did not provide a replacement for non fat-suppressed T1 images that are common in conventional protocols. In this study, structure delineation with T2Sh was not inferior to conventional 2D sequences. Nonetheless, in a number of cases 2D images were preferred, most notably in depicting the anterior/posterior tibiofibular and talofibular ligaments. This may be due to the lower SNR at the short TR, and may necessitate further tuning to determine the best reconstruction parameters. Inter-observer agreement was relatively low, likely due to readers’ inexperience with the T2Sh sequence. A limitation of the study was that structured reports were not compared to diagnostic reports. A second limitation was the small study size. A third limitation was that the readers were not blinded to image type.Conclusion
A single-sequence pediatric ankle exam is feasible with T2Sh, providing multiplanar, reformattable 4D images.Acknowledgements
We thank the following funding sources: National Institutes of Health (NIH) grants R01EB009690, P41RR09784; Sloan Research Fellowship; Bakar Fellowship; GE Healthcare, and Intel Labs.References
- SR Duc, et al., “Improved visualization of collateral ligaments of the ankle: multiplanar reconstructions based on standard 2D turbo spin-echo MR images”, Eur Radiol 17(5):1162–1171 (2007).
- V Kalia et al. “CAIPIRINHA accelerated SPACE enables 10-min isotropic 3D TSE MRI of the ankle for optimized visualization of curved and oblique ligaments and tendons”, Eur Radiol, 27:3652-3661 (2017).
- B Fritz, et al. “CAIPIRINHA-accelerated 10-min 3D TSE MRI of the ankle for the diagnosis of painful ankle conditions: Performance evaluation in 70 patients”, Eur Radiol (2018). https://doi.org/10.1007/s00330-018-5591-zS
- Bao, et al., “Fast comprehensive single-sequence four-dimensionalpediatric knee MRI with T2 shuffling”, J Magn Reson Imaging, 45(6):1700–1711 (2017).
- RF Busse, et al. "Effects of refocusing flip angle modulation and view ordering in 3D fast spin echo", Magn Reson Med, 60:640-9 (2008).
- JI Tamir, et al. “T2 shuffling: Sharp, multicontrast, volumetricfast spin-echo imaging”, Magn Reson Med, 77(1):180–195 (2017).
Figures