0130
Added Clinical Value of Isotropic MAVRIC SL Acquisitions of Total Hip Arthroplasties1Hospital for Special Surgery, New York, NY, United States, 2MR Applications and Workflow, GE Healthcare, Waukesha, WI, United States
Synopsis
MAVRIC SL, a multi-spectral MRI imaging sequence, reduces metallic susceptibility artifact to improve visualization near joint arthroplasty by acquiring 24 spectral bins of off-resonance data. Many implants require fewer bins, and this study uses a calibration scan to determine the number of bins necessary to permit an isotropic MAVRIC acquisition and a reduced TR isotropic MAVRIC acquisition. The isotropic MAVRIC images decreased blurring and improved visualization of the periprosthetic bone and synovium while retaining image quality. Lowering the TR decreased scan time but affected image interpretation. Isotropic MAVRIC acquisitions may improve the diagnostic capability of MAVRIC SL images.
Introduction
MAVRIC SL (MVSL) is a novel 3D multi-spectral image acquisition that reduces metallic susceptibility artifact and improves visualization of soft tissues surrounding total joint arthroplasty. It acquires data from 24 frequency bins (± 12 kHz) offset from the central hydrogen frequency, and the data are combined to generate output images (1). Acquiring a full set of data from 24 bins is excessive for weaker susceptibility orthopaedic implants that create smaller frequency dispersions (2). The number of bins necessary for adequate spectral coverage of a specific implant can be determined through a short spectral calibration scan (2), and the time savings can be used to acquire thinner slices with isotropic voxels (3). Scan times may be further reduced by decreasing the TR to a minimum value determined by the scanner based on the spectral calibration scan. This study expands upon previous work (3) that evaluated isotropic MAVRIC SL images to also include an isotropic MAVRIC SL acquisition with a scanner defined TR. The results will further elucidate the clinical benefit of isotropic acquisitions.Methods
This study was IRB approved. 47 patients (49 total hip arthroplasties) were enrolled: 20M/27F, 67.7 ± 10.4 y.o.. Images were generated using a clinical 1.5T scanner (GE Healthcare) with an 8 channel cardiac coil (Invivo). A calibration scan determined the number of spectral bins needed (2) (Matrix:128x32x24, TE/TR:7.2ms/1.4s, slice thickness:6mm, FOV:36-40cm, ETL:16, scan time:~35s). A 3D MAVRIC SL series (MVSL, TE/TR:8/4500ms, BW:±125kHz, FOV:38-44cm, Matrix:512x256, Slice Thickness:3.5mm, ETL:24, NEX:0.5) and an isotropic MAVRIC series (MVISO, TE/TR:8/3000ms, BW:±125kHz, FOV:38-44cm, voxel size:1.3mm3, ETL:48, NEX:0.5) were acquired. Additionally, an isotropic AutoTR MAVRIC SL series (AUTOMVISO) was acquired for 10 hips. The parameters for the AUTOMVISO were identical to the MVISO but used a scanner defined minimum TR to be within the range of 2500-3500ms.
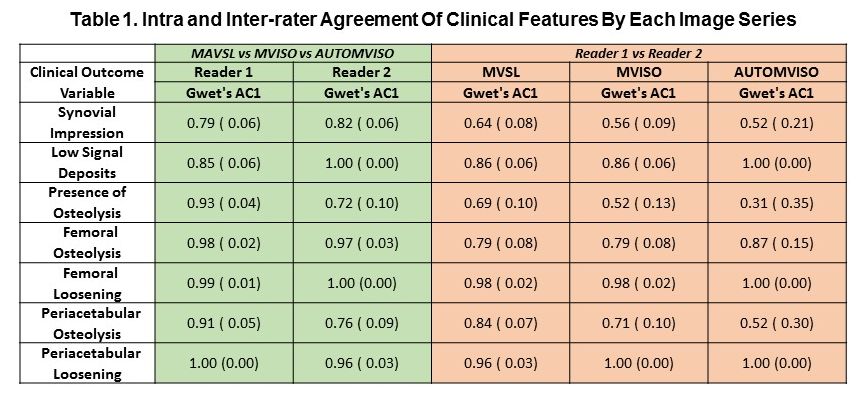
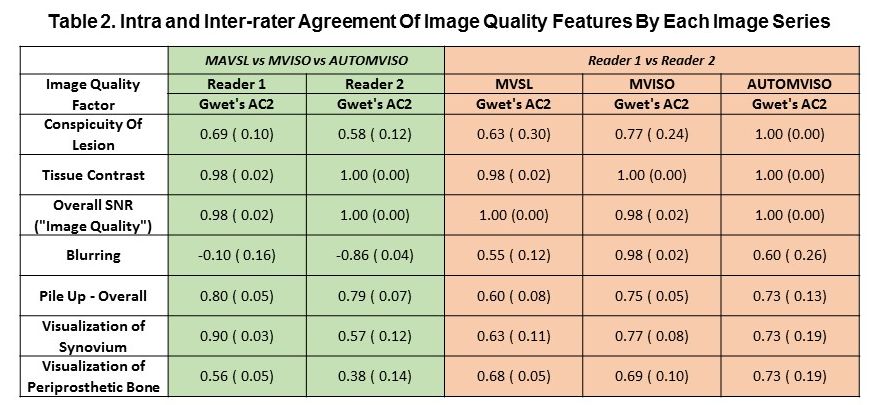
Images were blinded and individually evaluated by 2 board certified radiologists for the presence of low signal intensity deposits, osteolysis, loosening, and synovial response classification. Images were also evaluated qualitatively for lesion conspicuity, tissue contrast, blurring, artifact pile-up, visualization of the synovium and periprosthetic bone, and overall quality. Grades were assigned using the scale: 1-poor/severe, 2-decent/moderate, 3-good/mild-none. Image quality among the three image acquisitions was compared using a mixed effects ordinal logistic regression model. Inter/intra-rater agreement across images was determined using Gwet’s agreement coefficient (AC1 for unweighted and AC2 for ordinal weighted agreement). Mean scan times were estimated, and significance was set at p<0.05.
Results
The spectral calibration scan enabled the use of fewer bins (median: 14, range: 6-20). Mean AUTOMVISO scan times (5m33s±13s) were similar to MVSL scan times (5m51s±6s), and both were shorter than MVISO scan times (7m28s±6s, p<0.001). The radiologists had substantial to almost perfect inter-rater agreement for each image acquisition for a majority of clinical outcomes (16/21, 76%) and image quality outcomes (18/21, 86%, Tables 1,2). Inter-reader agreement of image quality outcomes depended on the type of acquisition, with reduced agreement found for conspicuity of lesion, blurring, and visualization of synovium and periprosthetic bone (Table 2) for MVSL images. Inter-reader clinical outcomes also depended on the acquisition, with reduced agreement found for synovial impression, presence of osteolysis, and detection of peri-acetabular osteolysis for AUTOMVISO imaging (Table 1).
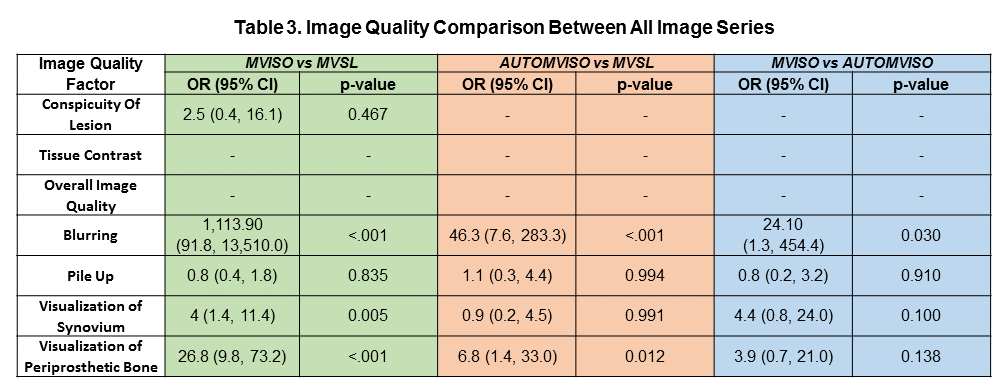
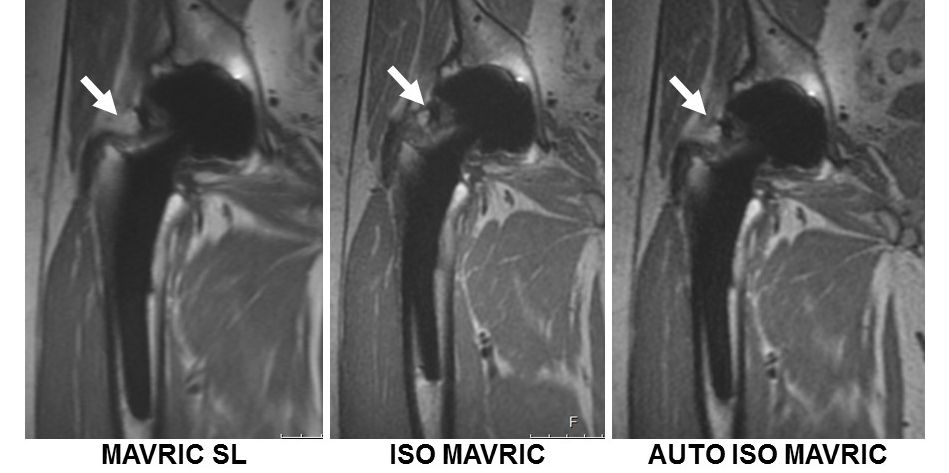
Isotropic acquisitions had
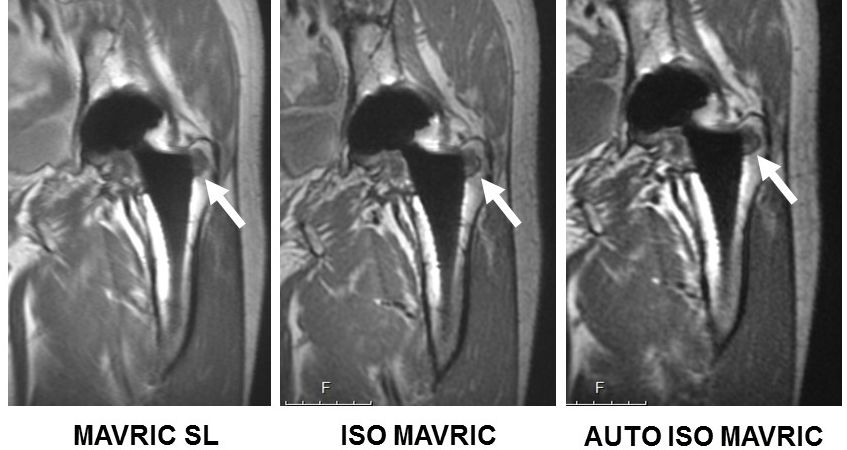
less blurring than MVSL (MVISO: Odds Ratio (OR)=1113.9, 95%CI:91.8-13,510,
p<0.001; AUTOMVISO: OR=46.3, 95%CI:7.6–283.3, p<0.001, Table 3, Figures 1,2).
In addition, MVISO reduced blurring more than AUTOMVISO (OR=24.0, 95%CI:1.3–454.4,
p=0.03, Table 3). MVISO images improved visualization of the synovium (OR=4, 95%CI:1.4–11.4,
p=0.005) and the periprosthetic bone (OR=26.8, 95%CI:9.8–73.2, p<0.001) over
MVSL images, and AUTOMVISO images also improved visualization of the
periprosthetic bone (OR=6.8, 95%CI:1.4–33, p=0.012) (Figure 2). MVISO and
AUTOMVISO had similar display of synovium and periprosthetic bone.
Discussion
The MVISO and AUTOMVISO series displayed several clinically relevant features better than MVSL images, with notable improvement of blurring and visualization of periprosthetic bone. Although AUTOMVISO imaging decreased blurring and improved visualization of periprosthetic bone over MVSL, it did not improve synovial visualization, as reflected in the low value of inter-rater agreement. We believe that decreasing the TR value to a scanner defined value altered the image contrast and contributed to the poorer visualization of synovial reactions. The study demonstrated that isotropic MAVRIC scans are clinically feasible, and that MVISO scans added clinical value through improved visualization by reducing blurring.Conclusions
Using a calibration scan successfully decreases the number of bins needed to generate high resolution images surrounding implants, and the reduction in scanning time affords the ability to acquire isotropic images that improve visualization of the implant while maintaining overall image quality. AutoTR isotropic MAVRIC scans reduced acquisition time but may affect image interpretation.Acknowledgements
HSS has an institutional research agreement in place with GE Healthcare. Research reported in this publication was partially supported by NIH/NIAMS R01AR064840.References
1. Koch KM, Lorbiecki JE, Hinks RS, King KF. A multispectral three-dimensional acquisition technique for imaging near metal implants. Magn Reson Med. 2009;61:381-390.
2. Kaushik SS, Marszalkowski C, Koch KM. External calibration of the spectral coverage for three-dimensional multispectral MRI. Magn Reson Med. 2016;76:1494-1503.
3. Koff MF, Kaushik S, Shah P, Argentieri E, Potter HG. Clinical Feasibility of Isotropic MAVRIC SL Imaging of Total Joint Arthroplasties. #331, Int'l Soc. Mag. Res. Med.2018; Paris, France.
Figures