0107
5-Minute Double-Echo in Steady-State with Separated Echoes for Comprehensive Whole-Joint Knee MRI Assessment with and without a Proton-Density-Weighted Sequence1Department of Radiology, Stanford University, Stanford, CA, United States, 2Department of Bioengineering, Stanford University, Stanford, CA, United States, 3LVIS Corporation, Palo Alto, CA, United States, 4Athinoula A. Martinos Center for Biomedical Imaging, Massachusetts General Hospital, Charlestown, MA, United States, 5Department of Radiology, Harvard Medical School, Boston, MA, United States, 6Department of Orthopaedic Surgery, Stanford University, Stanford, CA, United States, 7Department of Radiology & Nuclear Medicine, Erasmus MC, University Medical Center, Rotterdam, Netherlands, 8Department of Electrical Engineering, Stanford University, Stanford, CA, United States, 9Department of Neurology & Neurological Sciences, Stanford University, Stanford, CA, United States, 10Department of Neurology, Stanford University, Stanford, CA, United States
Synopsis
Most knee MRI protocols require 20+ minutes of scan time, leading to interest in expedited protocols. Here, we first demonstrate in a study with 35 patients and 5 readers that for diagnostic knee MRI, a 3D 5-minute quantitative double-echo steady-state (qDESS) sequence has high agreement with the conventional sequences, where the addition of a proton-density-weighted sequence engenders near-perfect agreement. In a second study with 51 patients and 2 readers, we demonstrate that qDESS with two-fold enhanced slice resolution using deep-learning-based super-resolution and T2 maps has high agreement with the conventional sequences, where both methods have similar agreement with arthroscopic findings.
Purpose
Most diagnostic knee MRI protocols require 20+ minutes of scan time, leading to great interest in expedited protocols1–3. A single 5-minute 3D quantitative double-echo in steady-state (qDESS) sequence can produce high-resolution and multi-contrast images with T1/T2-weighting (S+) and T2-weighting (S-), and quantitative T2 relaxation time maps4,5. This study compared the performance of a 5-minute qDESS sequence as a standalone technique, or paired with one sequence form the conventional MRI protocol, or enhanced with deep learning for diagnostic knee MRI.Methods
Thirty-five symptomatic patients (18 male, 17 female, age 43±19 years) scanned with a routine knee MRI protocol were scanned with sagittal 3D qDESS4 on a Discovery MR750 3.0T MRI scanner (GE Healthcare, Wisconsin) with an 8-channel transmit-receive knee coil (InVivo, Florida).
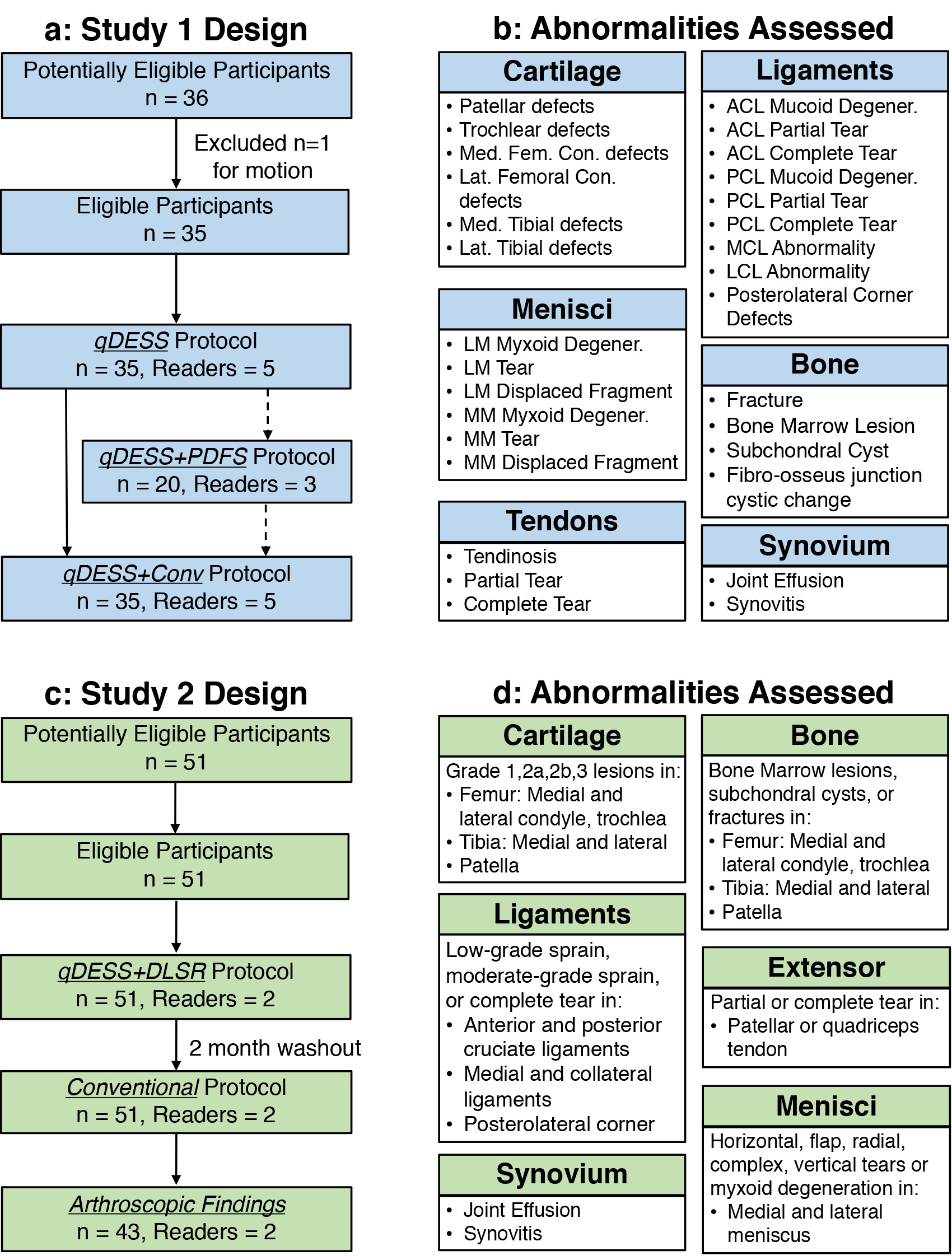
Five musculoskeletal radiologists evaluated all images for the presence of thirty common imaging findings in internal derangement of the knee, sub-divided into bone, cartilage, ligaments, menisci, synovium, and tendons (Fig.1). The readers recorded the presence of all findings (Yes/No) and scored the diagnostic confidence of the protocol used (0=None, 1=Low, 2=Moderate, and 3=High).
All readers first scored the qDESS-only protocol, and subsequently, qDESS combined with the conventional (qDESS+Conv protocol). In a subset of 20 patients, three of the five readers scored the qDESS protocol first, then qDESS-only with an additional coronal proton-density-weighted fat-saturated sequence (qDESS+PDFS protocol), and finally qDESS+Conv. The percentage of observations where qDESS-only or qDESS+PDFS had equivalent confidence as qDESS+Conv were tested with exact symmetry tests. Krippendorff's alpha (KA) coefficients evaluated inter-observer agreement6. Positive (PPA) and negative (NPA) percentage agreement and their confidence intervals (CI) for the qDESS-only and qDESS+PDFS protocols were calculated and differences between the qDESS-only and qDESS+PDFS measurements were tested by exact McNemar tests.
In a follow-up study, we utilized deep-learning super-resolution (DLSR) to enhance qDESS slice resolution twofold (from 1.6mm to 0.8mm) to mitigate multi-planar reformat (MPR) blurring7,8. 51 additional symptomatic patients (34 male, 17 female, age 44±18 years) were scanned with the same qDESS-only protocol and enhanced with DLSR. Two musculoskeletal radiologists assessed these qDESS+DLSR morphological images and T2 relaxation time maps, and the conventional protocol (with a 2 month washout period) for detecting abnormalities in ligaments, cartilage, meniscus, bone, extensor mechanism, and synovium (Fig.1). PPA and NPA was compared to the conventional protocol, while arthroscopic sensitivity and specificity comparisons were made for cartilage, meniscus, and ligament abnormalities. Both study schematics are shown in Fig.1.
Results
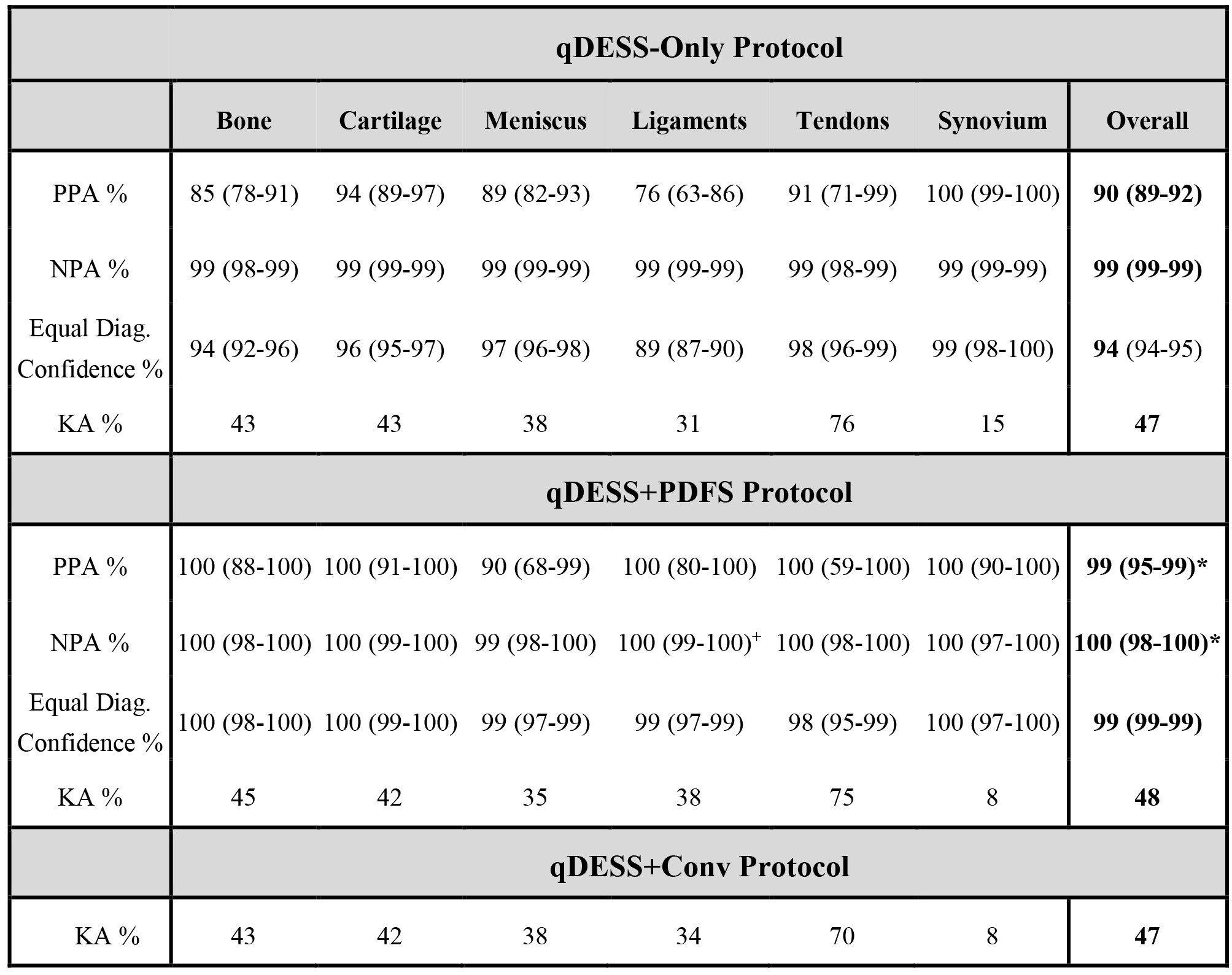
qDESS-only had equivalent diagnostic confidence as qDESS+Conv in 94% of findings compared to 99% for qDESS+PDFS (Fig.2). qDESS-only had a PPA of 90% (88-92% CI) and NPA of 99% (99-99% CI). qDESS+PDFS significantly increased PPA to 99% (95-99% CI) and NPA to 100% (99-100% CI) compared to qDESS-only (p<0.001). KA values of 47-48% for all three protocols indicated moderate inter-reader agreement9.
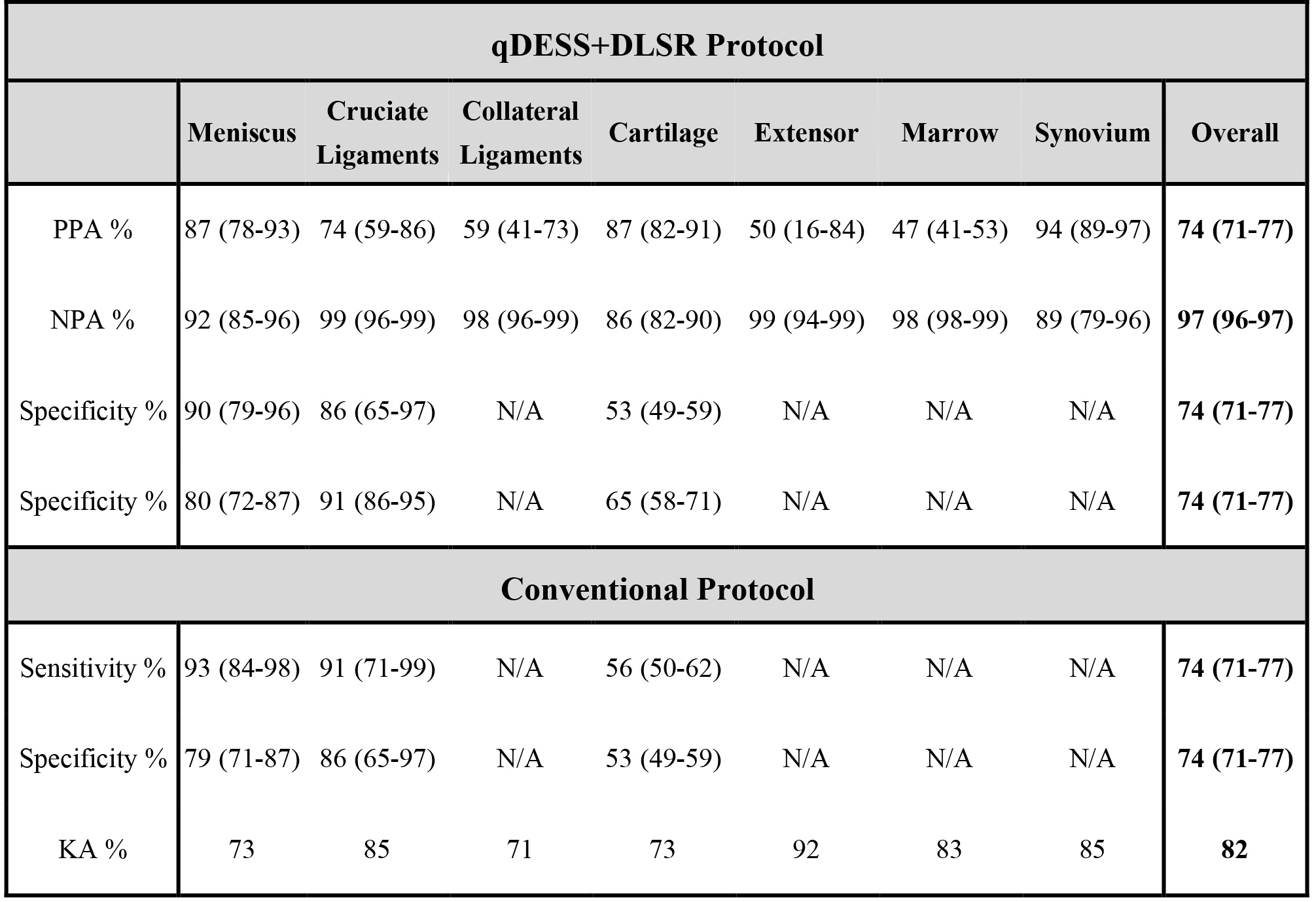
qDESS+DLSR generated 74% (71-77% CI) PPA and 97% (96-97% CI) NPA compared to the conventional protocol findings respectively (Fig.3). Overall qDESS+DLSR sensitivity and specificity for meniscal, ligament, and cartilage abnormalities was 61% (56-66% CI) and 76% (72-80% CI) respectively, which was comparable to 65% (60-70% CI) and 78% (74-81% CI) for the conventional protocol. There was high inter-reader agreement (Kappa=0.82). The presence of a T2 map added additional diagnostic value in 41/51 patients and in 38% of cartilage sub-regions.
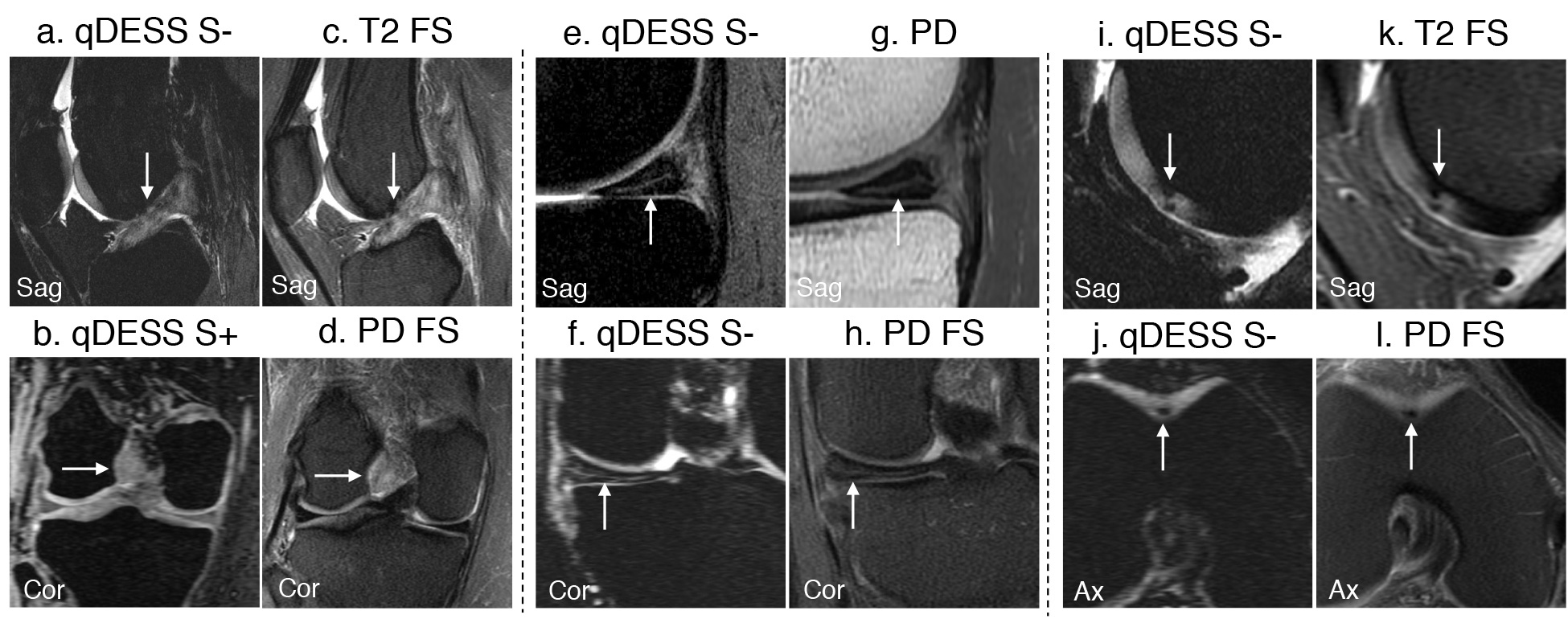
A full-thickness ACL tear, medial meniscus tear, and cartilage lesions in the femoral trochlea appeared similarly on qDESS-only images and the conventional images (Fig.4,5).
Discussion
qDESS-only had high diagnostic agreement and confidence compared to the conventional protocol. The qDESS+PDFS protocol addressed MPR blurring - a primary limitation of qDESS-only. The qDESS+DLSR follow-up study aimed to reduce MPR blurring by enhancing slice-resolution twofold. The high agreement of qDESS+DLSR with the conventional protocol in 51 patients, and similar arthroscopic comparisons as the conventional sequences suggests increased utility of qDESS without increased scan time.
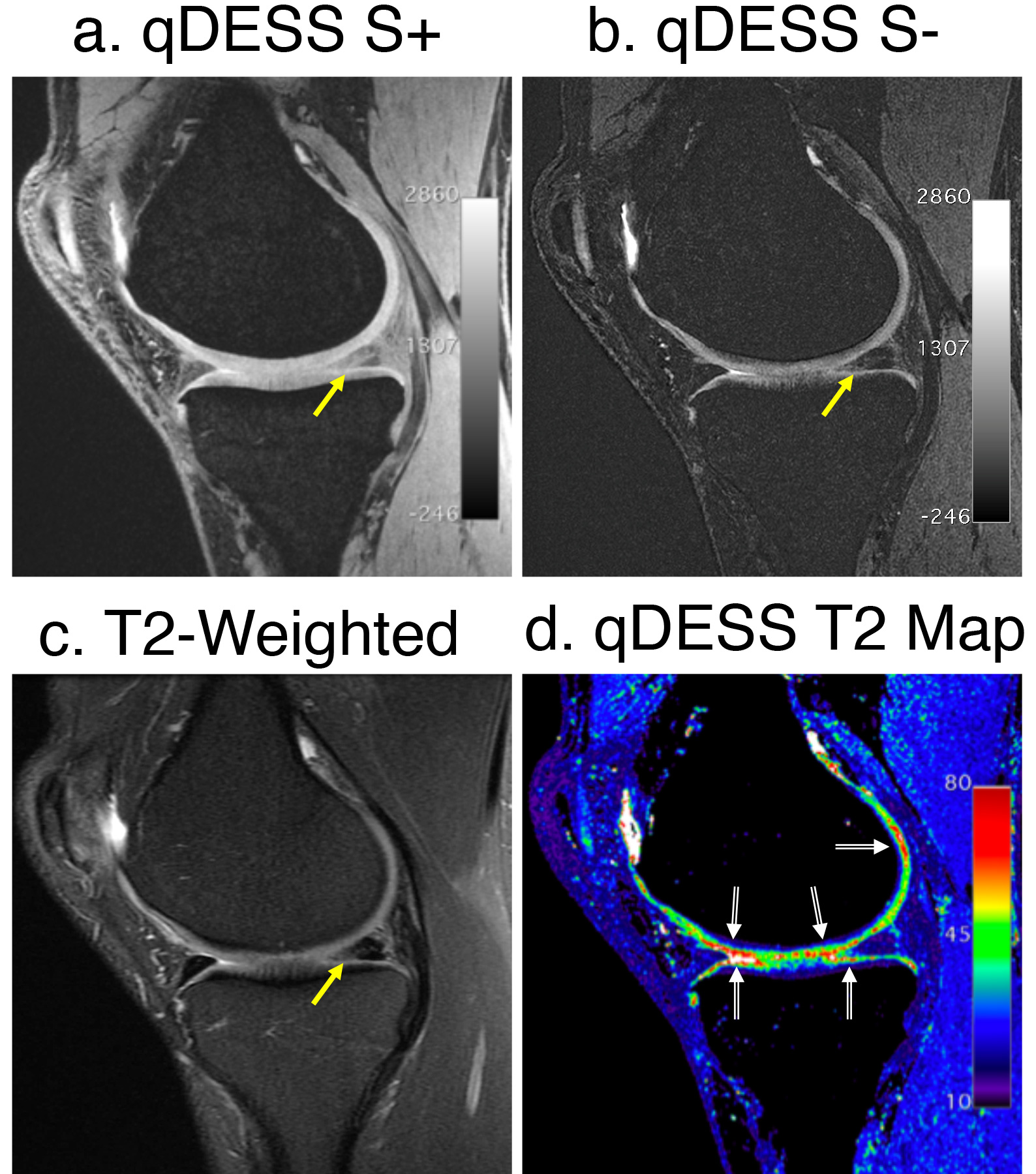
The 5-minute qDESS acquisition also has similar morphometry and T2 relaxometry performance compared to validated 20+ minute protocols, which may enable acquiring quantitative osteoarthritis biomarkers from diagnostic scans4,10. The explicit use of T2 maps diagnostically (Fig. 5) may detect early tissue degeneration, prior to morphological changes. Novel fully-automated and accurate cartilage segmentation and visualization techniques may enable using T2 measurements in routine practice11–13. Simultaneous bilateral knee MRI with qDESS is also possible without a loss in image quality and quantitative accuracy, for further enhancing efficiency14.
Conclusion
We have combined advanced acquisition, quantitative imaging, and deep learning to use a 5-minute qDESS sequence as a standalone technique, or paired with PDFS, or enhanced with DLSR, to perform rapid and accurate diagnostic knee MRI.Acknowledgements
No acknowledgement found.References
- Bao S, Tamir JI, Young JL, et al. Fast comprehensive single-sequence four-dimensional pediatric knee MRI with T2 shuffling. J Magn Reson Imaging. October 2016:1-12. doi:10.1002/jmri.25508.
- Del Grande F, Delcogliano M, Guglielmi R, et al. Fully Automated 10-Minute 3D CAIPIRINHA SPACE TSE MRI of the Knee in Adults. Invest Radiol. 2018;00(00):1. doi:10.1097/RLI.0000000000000493.
- Kijowski R, Rosas H, Samsonov A, King K, Peters R, Liu F. Knee imaging: Rapid three-dimensional fast spin-echo using compressed sensing. J Magn Reson Imaging. 2017;45(6):1712-1722. doi:10.1002/jmri.25507.
- Chaudhari AS, Black MS, Eijgenraam S, et al. Five-minute knee MRI for simultaneous morphometry and T 2 relaxometry of cartilage and meniscus and for semiquantitative radiological assessment using double-echo in steady-state at 3T. J Magn Reson Imaging. 2018;47(5):1328-1341. doi:10.1002/jmri.25883.
- Chaudhari AS, Stevens KJ, Sveinsson B, et al. Combined 5-minute double-echo in steady-state with separated echoes and 2-minute proton-density-weighted 2D FSE sequence for comprehensive whole-joint knee MRI assessment. J Magn Reson Imaging. 2018:1-12. doi:10.1002/jmri.26582.
- Krippendorf K. Reliability in content analysis: Some common misconceptions and recommendations. Hum Commun Res. 2004;30(3):411-433. doi:http://dx.doi.org/10.1111/j.1468-2958.2004.tb00738.x.
- Chaudhari A, Fang Z, Lee JH, Gold G, Hargreaves B. Deep Learning Super-Resolution Enables Rapid Simultaneous Morphological and Quantitative Magnetic Resonance Imaging. In: International Workshop on Machine Learning for Medical Image Reconstruction. ; 2018:3-11. http://arxiv.org/abs/1808.04447.
- Chaudhari AS, Fang Z, Kogan F, et al. Super-resolution musculoskeletal MRI using deep learning. Magn Reson Med. 2018. doi:10.1002/mrm.27178.
- Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977;33(1):159-174. doi:10.2307/2529310.
- Peterfy CG, Schneider E, Nevitt M. The osteoarthritis initiative: report on the design rationale for the magnetic resonance imaging protocol for the knee. Osteoarthr Cartil. 2008;16(12):1433-1441. doi:10.1016/j.joca.2008.06.016.
- Norman B, Pedoia V, Majumdar S. Use of 2D U-Net Convolutional Neural Networks for Automated Cartilage and Meniscus Segmentation of Knee MR Imaging Data to Determine Relaxometry and Morphometry. Radiology. 2018;000(0):172322. doi:10.1148/radiol.2018172322.
- Desai AA, Gold GE, Hargreaves BA, Chaudhari AS. Technical Considerations for Semantic Segmentation in MRI using Convolutional Neural Networks. arXiv Prepr arXiv190201977. 2019.
- Monu UD, Jordan CD, Samuelson BL, Hargreaves BA, Gold GE, McWalter EJ. Cluster Analysis of Quantitative MRI T2 and T1ρ Relaxation Times of Cartilage Identifies Differences between Healthy and ACL-injured Individuals at 3T. Osteoarthr Cartil. 2016;25(October):1-8. doi:10.1016/j.joca.2016.09.015.
- Kogan F, Levine EG, Chaudhari AS, et al. Simultaneous Bilateral-Knee MR Imaging. Magn Reson Med. 2017. doi:DOI 10.1002/mrm.27045.
Figures