0104
Ex-vivo MR-guided pathology to improve lymph node staging in rectal cancer1Radiology, Radboudumc, Nijmegen, Netherlands, 2Pathology, Canisius-Wilhelmina hospital, Nijmegen, Netherlands, 3Surgery, Radboudumc, Nijmegen, Netherlands, 4Pathology, Radboudumc, Nijmegen, Netherlands
Synopsis
Pathological lymph node yield can be influenced by multiple factors. The use of ex-vivo MR guided pathology of rectal specimens could provide insight in the number and size of lymph nodes present in a rectal specimen and aid in an increased pathological lymph node yield. Therefore two series of rectal specimens were examined, one control group and one MR-guided group. Ex-vivo MRI revealed significantly more and significantly smaller lymph nodes without increasing the pathological yield. Small nodes appear to be difficult to harvest, presumably requiring a 3D approach for further improvement of pathological evaluation.
Introduction
Presence of lymphatic spread in rectal cancer patients determines the treatment regimen. Histopathological evaluation is the gold standard in definite staging the disease. International guidelines prescribe a minimum pathological yield of 12 lymph nodes.1-3 However, there are many factors that can influence the yield such as age, surgery and preoperative (chemo)radiotherapy.4,5 Multiple studies have aimed to improve the pathologic lymph node yield, but there are no studies focusing on the use of ex-vivo MRI.6-9 MRI is known to be the superior 3D imaging modality with high spatial resolution to identify and characterize lymph nodes in-vivo.10 By applying 7 Tesla ex-vivo MRI to rectal specimens, high spatial resolution imaging can visualize all lymph nodes present in the specimen.11 These images then can be used to guide the pathologist towards these lymph nodes. In this study, we aim to use 7 Tesla ex-vivo MRI scans to determine the size of lymph nodes and to increase the pathologic yield after MR-guided pathology.Methods
This prospective, observational study evaluated the added value of MR-guided pathology for harvesting lymph nodes in two series of rectal cancer specimens. The first series (S1) was examined to establish the number and size of lymph nodes separately on ex-vivo MRI and on histopathology. Lymph nodes detected on ex-vivo MRI of the second series (S2) were used to guide the pathologist during pathologic examination. The number, size and percentages of yielded lymph nodes of S1 and S2 were then compared. Fixated rectal specimens were scanned in a 7 Tesla pre-clinical MRI system (ClinScan, Bruker® BioSpin, Ettlingen, Germany). The MR protocol consisted of a T1-weighted 3D gradient echo (GRE) sequence with lipid excitation (TR/TE 15/3 ms, resolution 0.293 mm3) and a water-excited 3D multi-GRE (TR 30 ms, computed TE 6.2ms, resolution 0.293 mm3). Annotations were drawn around the lymph nodes on lipid and water selective GRE images. MR-guided pathology for S2 was performed by using the annotations on ex-vivo MRI during macroscopic examination (figure 1).Results
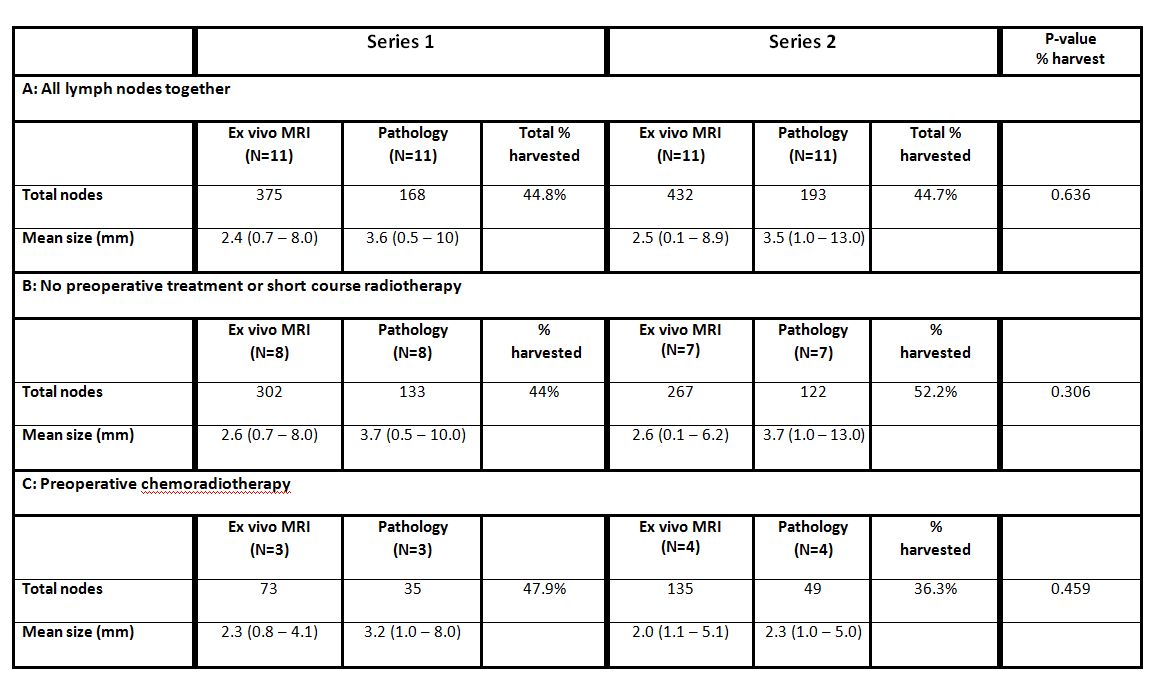
Twenty-two rectal specimens were included, subdivided in 11 specimens per series. Relevant characteristics are displayed in table 1. The median number of harvested lymph nodes did not significantly differ between the two series. Overall, a mean number of 37 (range 16–76) and 16 (range 4–30) lymph nodes per specimen were revealed on ex-vivo MRI and histopathology, respectively. This difference in yield was significant for both series (p=0.003). Numbers and size for detected lymph nodes on ex-vivo MRI and during pathological examination for both series are represented in table 2. Mean size of all lymph nodes did not differ between the two series (ex-vivo MRI: 2.4 vs. 2.5mm, p=0.267; pathology: 3.6 vs. 3.5mm, p=0.653). Preoperative treatment had no influence on the proportion and size of harvested lymph nodes. Size distributions are graphically displayed in figure 2. Figure 3A illustrates the percentages of harvested lymph nodes compared to nodes visible on ex-vivo MRI per specimen for both series. By using a size threshold of >2mm (figure 3B), the percentage improved from 40 to 71% (S1) and from 43 to 78% (S2).Discussion
The current study showed that there is no effect of MR-guidance on the number and size of lymph node harvest from a rectal specimen. A remarkable finding was that ex-vivo MRI visualized significantly more and significantly smaller lymph nodes than those yielded during pathological examination. The hypothesis that small lymph nodes would be more easily detectable using MR-guided pathology was not confirmed, illustrated by the results of the lymph node harvest after using a threshold of >2mm. The question arises what those <2mm MR structures could be, apart from lymph nodes. Multiple microscopic cross sections of tissue fragments supposingly containing lymph nodes based on MRI, revealed some vascular structures, nerve branches, or only lipid tissue. Representations of tubular structures such as vessels and nerves are easily differentiated from the appearance of lymph nodes on MRI by simultaneous evaluation of transverse, sagittal and coronal images. The 3D visualization make it unlikely to mistake lymph nodes for tubular structures. It seems plausible that the translation from a 3-dimensional MR dataset to a 2-dimensional approach as the pathological evaluation is more challenging than presumed. This subsequently can result in missing lymph nodes below a certain size.Conclusion
Ex-vivo MRI visualizes more lymph nodes than (MR-guided) pathology is able to harvest. Current pathological examination is not further improved by MR-guidance. The majority of spherical structures below 3 mm in size remains unexplained, which warrants a 3D approach for pathological reconstruction of specimens.Acknowledgements
No acknowledgement found.References
1. Sobin LH, Greene FL. TNM classification: clarification of number of regional lymph nodes for pNo. Cancer 2001;92:452. 2. Awwad GE, Tou SI, Rieger NA. Prognostic significance of lymph node yield after long-course preoperative radiotherapy in patients with rectal cancer: a systematic review. Colorectal disease : the official journal of the Association of Coloproctology of Great Britain and Ireland 2013;15:394-403. 3. Sobin LH, Gospodarowicz M.K., Wittekind C. TNM classification of malignant tumours. 7th edition. Wiley-Blackwell 2009. 4. Mechera R, Schuster T, Rosenberg R, Speich B. Lymph node yield after rectal resection in patients treated with neoadjuvant radiation for rectal cancer: A systematic review and meta-analysis. European journal of cancer (Oxford, England : 1990) 2017;72:84-94. 5. Gravante G, Parker R, Elshaer M, et al. Lymph node retrieval for colorectal cancer: Estimation of the minimum resection length to achieve at least 12 lymph nodes for the pathological analysis. International journal of surgery (London, England) 2016;25:153-7. 6. Markl B, Kerwel TG, Wagner T, Anthuber M, Arnholdt HM. Methylene blue injection into the rectal artery as a simple method to improve lymph node harvest in rectal cancer. Modern pathology : an official journal of the United States and Canadian Academy of Pathology, Inc 2007;20:797-801. 7. Reima H, Saar H, Innos K, Soplepmann J. Methylene blue intra-arterial staining of resected colorectal cancer specimens improves accuracy of nodal staging: A randomized controlled trial. European journal of surgical oncology : the journal of the European Society of Surgical Oncology and the British Association of Surgical Oncology 2016;42:1642-6. 8. Markl B, Kerwel TG, Jahnig HG, et al. Methylene blue-assisted lymph node dissection in colon specimens: a prospective, randomized study. American journal of clinical pathology 2008;130:913-9. 9. Borowski DW, Banky B, Banerjee AK, et al. Intra-arterial methylene blue injection into ex-vivo colorectal cancer specimens improves lymph node staging accuracy: a randomized controlled trial. Colorectal disease : the official journal of the Association of Coloproctology of Great Britain and Ireland 2014;16:681-9. 10. Al-Sukhni E, Milot L, Fruitman M, et al. Diagnostic accuracy of MRI for assessment of T category, lymph node metastases, and circumferential resection margin involvement in patients with rectal cancer: a systematic review and meta-analysis. Annals of surgical oncology 2012;19:2212-23. 11. Langman G, Patel A, Bowley DM. Size and distribution of lymph nodes in rectal cancer resection specimens. Diseases of the colon and rectum 2015;58:406-14.Figures
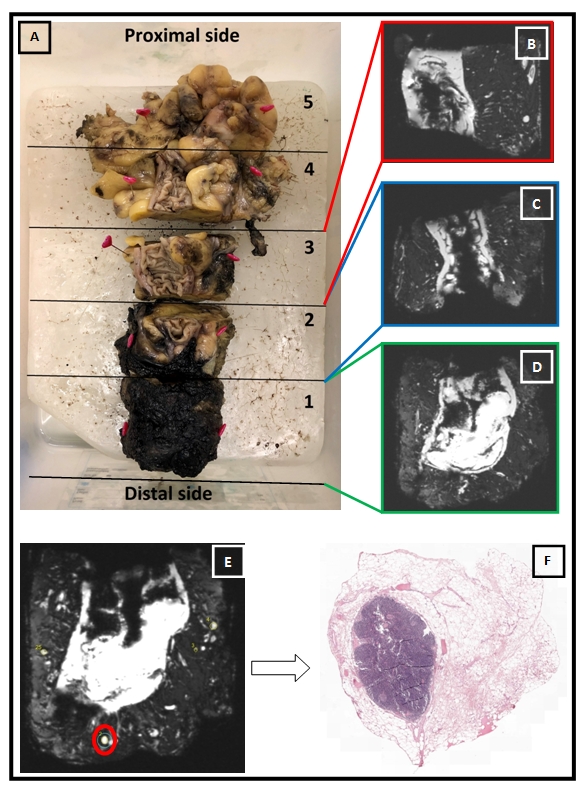


Figure 3A. Percentage of all lymph nodes harvested during pathologic assessment compared to annotated nodes on ex vivo MRI. The red bars represent the specimens of S1, the green bars represent the specimens of S2.
Figure 3B. Percentage of lymph nodes ≥ 2 mm harvested during pathologic assessment compared to annotated nodes on ex vivo MRI. The red bars represent the specimens of S1, the green bars represent the specimens of S2.