0102
The feasibility of matching lymph nodes detected on USPIO-enhanced MRI with histopathology in rectal cancerRutger C.H. Stijns1, Bart W.J. Philips1, Iris D. Nagtegaal2, Fatih Polat3, Johannes H.W. de Wilt4, Carla A.P. Wauters5, Patrik H.W. Zamecnik6, Jurgen J. Futterer1, and Tom W.J. Scheenen1
1Radiology, Radboudumc, Nijmegen, Netherlands, 2Pathology, Radboudumc, Nijmegen, Netherlands, 3Surgery, Cansius-Wilhelmina hospital, Nijmegen, Netherlands, 4Surgery, Radboudumc, Nijmegen, Netherlands, 5Pathology, Cansius-Wilhelmina hospital, Nijmegen, Netherlands, 6Radboudumc, Nijmegen, Netherlands
Synopsis
Lymph node staging in rectal cancer based on imaging is a major challenge. Node-to-node matching is crucial to determine the histopathology of lymph nodes that are detected on in-vivo MRI. A workflow of in-vivo MRI, ex-vivo MRI and MR-guided pathology was set up for lymph nodes that were characterized on USPIO-enhanced MRI. Difficulties were seen in the node-to-node matching, in despite of the use of high-resolution 3D ex-vivo MRI to link in-vivo detected nodes to final pathology.
Introduction
The presence of lymph node metastases in rectal cancer is a key factor in determining prognosis and treatment. Lymph node staging based on imaging, however, is still a major challenge.1.2 There is a need for a biomarker than can accurately predict the presence of lymph node metastases. Ferumoxtran-10, an ultrasmall superparamagnetic iron oxide (USPIO) particle, has proven to be a valuable contrast agent for detecting lymph node metastases.3-5 Previous studies were performed on 1.5 Tesla MR systems with known restrictions in resolution.6 By using 3-dimensional USPIO-enhanced MRI on a 3 Tesla MR system, it is possible to increase spatial resolution, thereby increasing the sensitivity for the detection of small suspicious nodes.7 Histopathological validation of these small lymph nodes on USPIO-enhanced MRI is crucial, and requires a method to match in-vivo detected nodes to final histopathology. In this abstract, initial results of a node-to-node matching of lymph nodes detected on USPIO-enhanced MRI in rectal cancer patients will be presented.Methods
The study is a prospective, diagnostic cohort study focusing on patients with rectal cancer who undergo total mesorectal excision (TME). Ferumoxtran-10 was administered with a dose of 2.6 mg/kg body weight. 24-36 hours later, MRI examination was performed at 3 Tesla (Magnetom® Prisma, Siemens Healthcare, Erlangen, Germany). The workflow of this study has previously been described.8 Detection of lymph nodes was done on T1-weighted MRI and on multi-gradient echo T2*-weighted MRI with reconstructed computed echo time of 12msec.9 USPIO-enhanced MR images were evaluated by 2 experienced radiologists (R1 and R2), using a classification scheme as illustrated in table 1.10,11 After surgery, fixated TME specimens were examined on a 7 Tesla preclinical MR system (ClinScan, Bruker® BioSpin, Ettlingen, Germany). Lymph nodes were annotated on ex-vivo MR images by a trained researcher and were used for MR-guided pathological examination. With the 3D image set at hand, the specimens were cut from distal to proximal by the pathologist; together with the trained researcher the locations of lymph nodes in the 3D MR images were used to harvest annotated lymph nodes (figure 1).Results
Ten patients have been included in this study. Five patients were scheduled for surgery and 5 patients for preoperative chemoradiotherapy followed by surgery. A total of 138 and 255 lymph nodes were annotated on in-vivo MRI by reader 1 (R1) and reader 2 (R2), respectively. All in-vivo detected nodes were classified according to their appearance on T2*w MRI (table 2) of which two examples are shown in figure 2. The median number of detected nodes per patient was 13.0 (range 7–24) versus 23.0 (range 15–54) (R1 vs. R2; p=0.005). On the ex-vivo MRI scans 428 lymph nodes with a mean size of 2.4 mm (range 0.7–8.0) were annotated and 216 lymph nodes were found at histopathology. From in-vivo MRI to ex-vivo MRI, a node-to-node match was possible in 70 lymph node and from ex-vivo MRI to histopathology 88 lymph nodes could be matched. A final direct node-to-node matching from in-vivo MRI to histopathology was possible for 43 lymph nodes detected by R1 and 37 of these matched with nodes detected by R2 (size distribution of these 37 nodes displayed in figure 3).Discussion
The current study design for node-to-node matching of in-vivo detected lymph nodes with histopathology shows that matching small lymph nodes in the mesorectum remains challenging, even with high resolution 3D ex-vivo MRI for guidance. Although the number of in-vivo detected nodes differed between the two readers, their interpretation of USPIO-enhanced MRI showed no great variations. Type 1 and type 7 lymph nodes were most frequently described during lymph node assessment. Difficulties regarding the matching process were encountered in both the steps from in-vivo MRI to ex-vivo MRI as well as in the translation from ex-vivo MRI to histopathology. This may be due to the large number of small nodes that become visible using (ultra-) high field MRI. Further in-depth analysis using a threshold for lymph nodal size possibly improves the relative amount of nodes that can be matched node-to-node. Moreover, pathological evaluation is a 2-dimensional examination which may be difficult to translate to a 3D representation created by MRI. For a higher matching rate, automation of pathological procedures into a full 3D pathological overview of the specimens is warranted. Future histopathological investigation will go into more detail on nodal types compared to pathological diagnosis.Conclusion
Even with high-resolution 3D ex-vivo MRI of resected specimens as an aid, node-to-node matching of in-vivo detected lymph nodes with histopathology in rectal cancer is a challenge.Acknowledgements
No acknowledgement found.References
1. Beets-Tan RGH, Lambregts DMJ, Maas M, et al. Magnetic resonance imaging for clinical management of rectal cancer: Updated recommendations from the 2016 European Society of Gastrointestinal and Abdominal Radiology (ESGAR) consensus meeting. European radiology 2017. 2. Elferink MA, Siesling S, Lemmens VE, et al. Variation in lymph node evaluation in rectal cancer: a Dutch nationwide population-based study. Annals of surgical oncology 2011;18:386-95. 3. Fortuin AS, Bruggemann R, van der Linden J, et al. Ultra-small superparamagnetic iron oxides for metastatic lymph node detection: back on the block. Wiley interdisciplinary reviews Nanomedicine and nanobiotechnology 2017. 4. Lahaye MJ, Beets GL, Engelen SM, et al. Locally advanced rectal cancer: MR imaging for restaging after neoadjuvant radiation therapy with concomitant chemotherapy. Part II. What are the criteria to predict involved lymph nodes? Radiology 2009;252:81-91. 5. Lahaye MJ, Engelen SM, Kessels AG, et al. USPIO-enhanced MR imaging for nodal staging in patients with primary rectal cancer: predictive criteria. Radiology 2008;246:804-11. 6. Harisinghani MG, Barentsz J, Hahn PF, et al. Noninvasive detection of clinically occult lymph-node metastases in prostate cancer. The New England journal of medicine 2003;348:2491-9. 7. Heesakkers RA, Futterer JJ, Hovels AM, et al. Prostate cancer evaluated with ferumoxtran-10-enhanced T2*-weighted MR Imaging at 1.5 and 3.0 T: early experience. Radiology 2006;239:481-7. 8. R.C.H. Stijns EWJP, I.D. Nagtegaal, F. Polat, L.J.A. Strobbe, J.H.W. de Wilt, C. Wauters, Stefan Rietsch, Sascha Brunheim, Stephan Orzada, Harald Quick, J.F. Fütterer, T.W.J. Scheenen. The workflow for the validation of USPIO-enhanced MRI for the detection of lymph node metastases in rectal cancer. 2018. 9. Philips BWJ, Fortuin AS, Orzada S, Scheenen TWJ, Maas MC. High resolution MR imaging of pelvic lymph nodes at 7 Tesla. Magnetic resonance in medicine 2017;78:1020-8. 10. Harisinghani MG, Saksena MA, Hahn PF, et al. Ferumoxtran-10-enhanced MR lymphangiography: does contrast-enhanced imaging alone suffice for accurate lymph node characterization? AJR American journal of roentgenology 2006;186:144-8. 11. Anzai Y, Piccoli CW, Outwater EK, et al. Evaluation of neck and body metastases to nodes with ferumoxtran 10-enhanced MR imaging: phase III safety and efficacy study. Radiology 2003;228:777-88.Figures
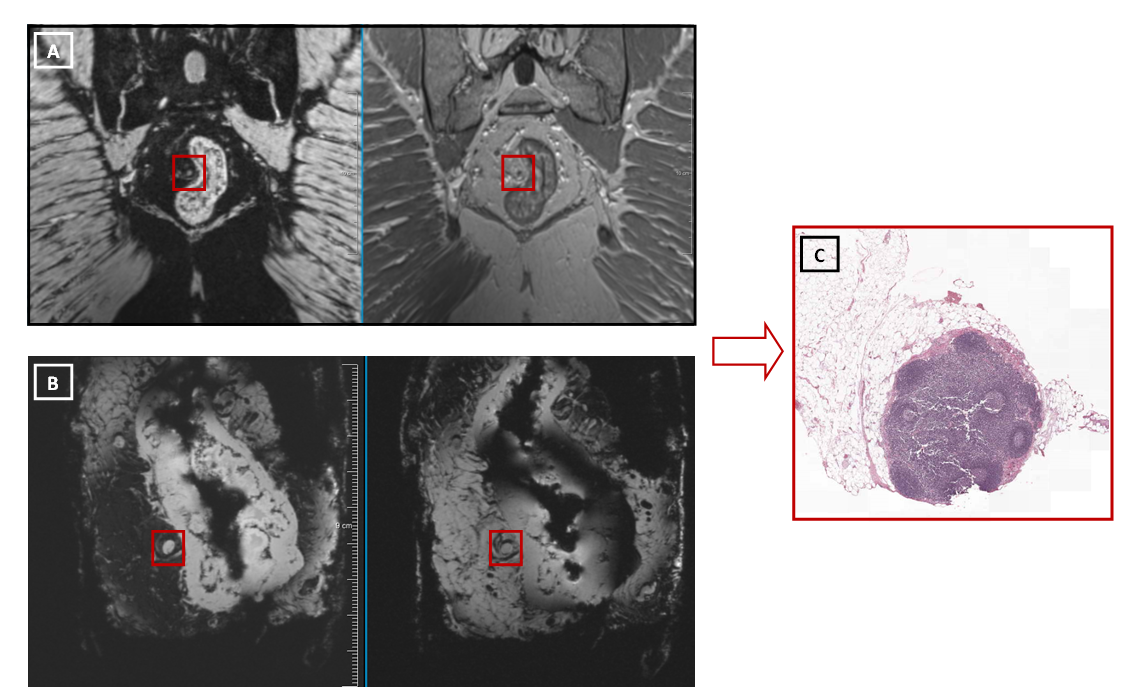
Example
of node-to-node matching from in vivo
MRI (A: left image displays the mGRE data; right image displays the VIBE DIXON
data) to ex vivo MRI (B: left image
displays the water selective data; right image displays the lipid selective
data) to pathological evaluation (C). In this example the specific location of
the lymph node close to the rectal wall as displayed on in vivo and ex vivo MRI
was used to locate the lymph node during pathologic evaluation.
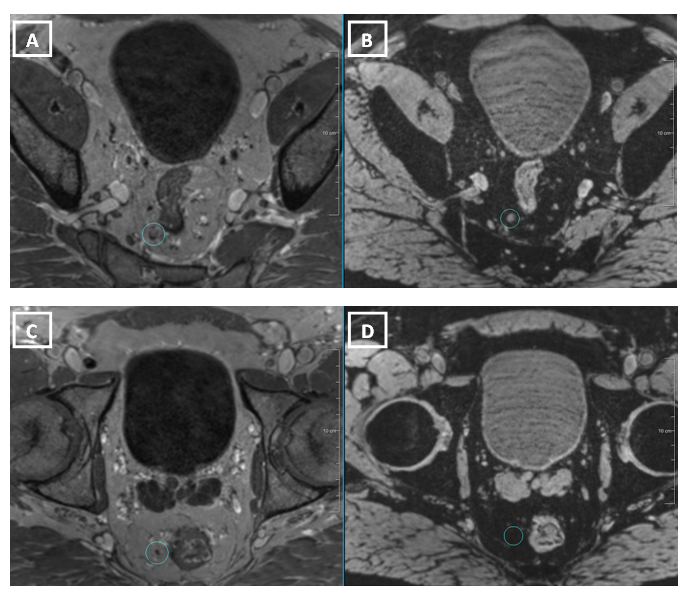
A
transverse image of a lymph node on
T1-weighted MRI (A) which was classified as nodal type 1 on the mGRE
T2*-weighted MRI with a computed echo time of 12 msec (B); and a transverse
image of a lymph node on T1-weighted MRI
(C) which was classified as nodal type 7 on the mGRE T2*-weighted MRI with a
computed echo time of 12 msec (D).
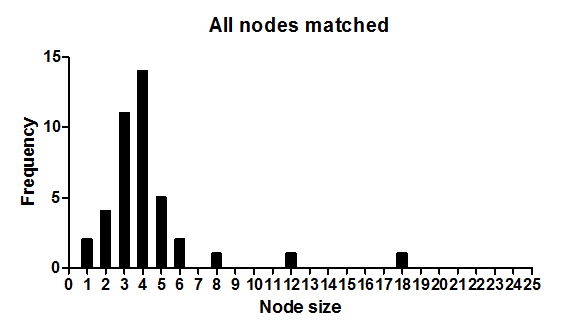
Size
distribution of the lymph nodes that could be matched from in-vivo MRI to histopathology
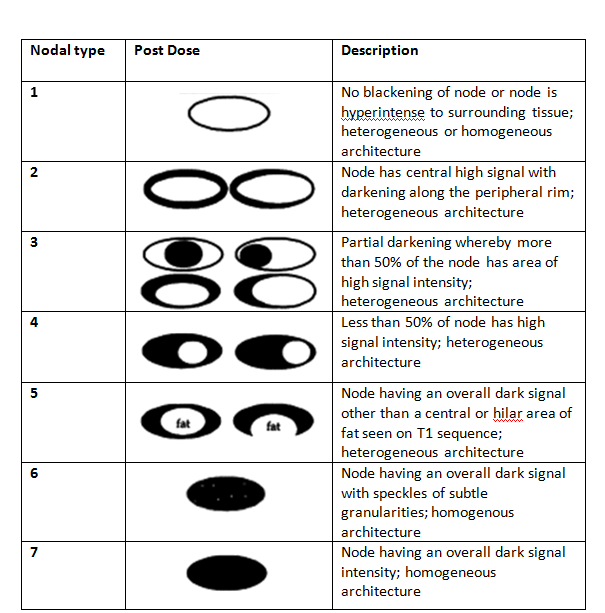
Nodal
classification scheme that was used for the assessment of lymph nodes that were
detected
on USPIO-enhanced MR images.
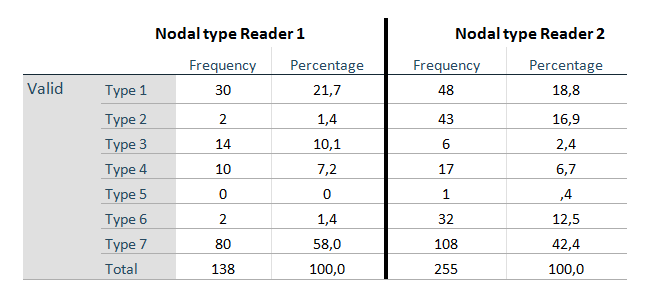
Overview
of the nodal types scored by reader 1 and 2 following the scheme of table 1.