0096
Technical Feasibility of Three-Dimensional Magnetic Resonance Elastography for Assessing Endometrial Carcinoma1Department of Radiology, The third affiliated hospital of Sun Yat-sen University, Guangzhou, China, 2Department of Radiology, Mayo Clinic, Rochester, MN, United States, 3MR Research China, GE Healthcare, Beijing, China
Synopsis
Endometrial carcinoma (EC) is one of the most common primary malignant tumors in women worldwide. Tumor grades, International Federation of Gynecology and Obstetrics (FIGO) stage and myometrial invasion of EC are important factors for treatment planning and prognosis. We explored the potential value of MR elastography (MRE) for the prediction of tumor grades, FIGO stage and myometrial invasion of EC. Our study showed that mean tumor stiffness may be a useful metric for differentiating well or moderately differentiated EC from poorly differentiated EC and for differentiating superficial invasion from deep myometrial invasion in EC.
Introduction
Endometrial carcinoma (EC) is the sixth most common malignant tumor in women worldwide1. The prognosis and treatment of patients with EC mainly depends on tumor grade, International Federation of Gynecology and Obstetrics (FIGO) stage and its depth of invasivation2. Magnetic resonance imaging (MRI) has long been considered an accurate technique for preoperative staging of EC. However, conventional MRI is not accurate when the tumor is large or occurs with endometriosis and fibroids3. Stiffness is an intrinsic mechanical property of the tissue and the occurrence of a tumor can increase the stiffness of the tissue4. Recently, MRE has been introduced as a method to evaluate tissue composition for various cancers, such as hepatocellular carcinoma, breast, pancreatic, and prostate cancer4-6. The purpose of this study was to evaluate the feasibility of trans-pelvic 3D MRE of the uterus and to assess the diagnostic performance of 3D MRE for determining tumor grades, FIGO stage and myometrial invasion of EC.Methods
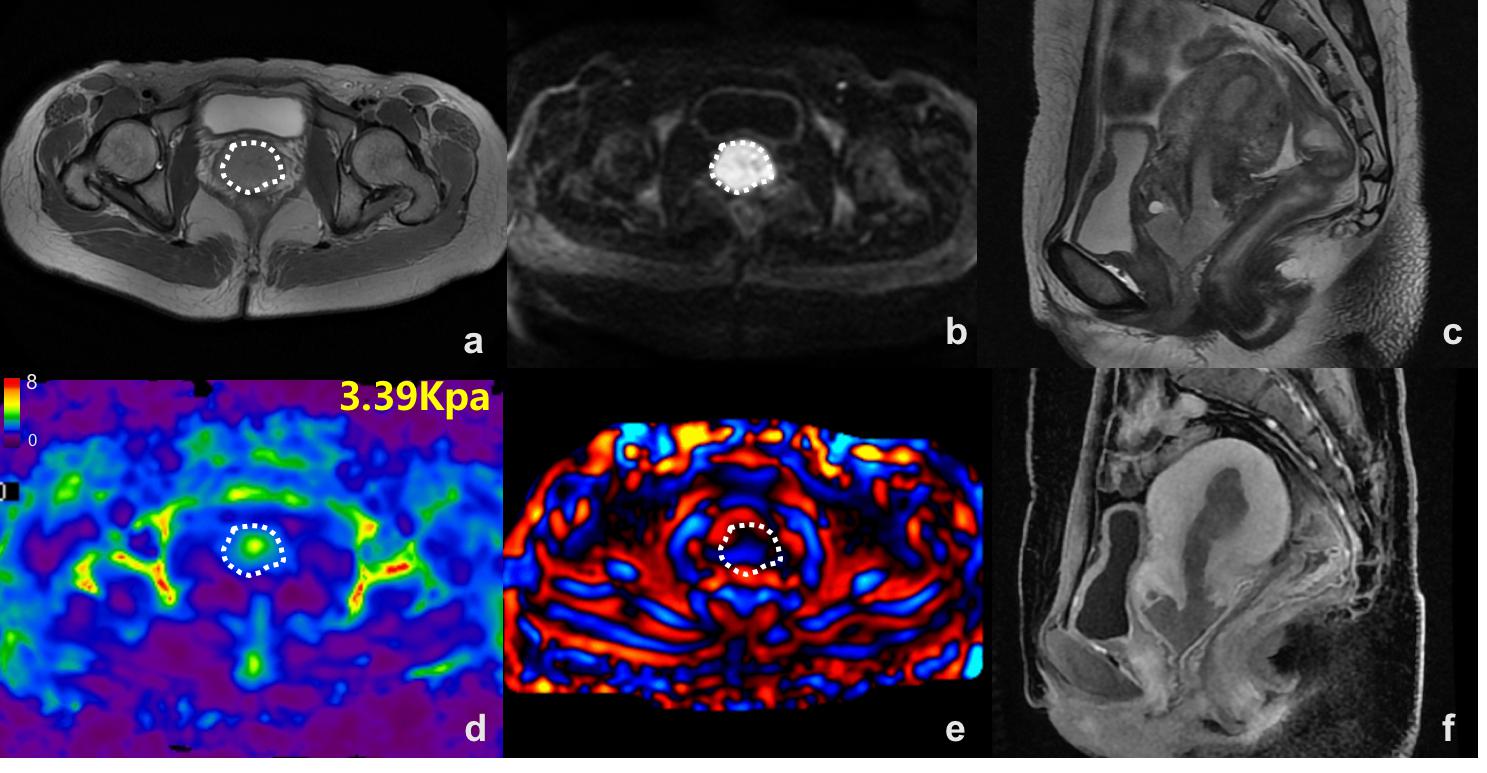
This retrospective study was approved by our institutional review board. A total of 22 patients with EC were initially enrolled who underwent trans-pelvic 3D MRE. 7 patients were excluded for the following reasons: failure of the MRE exam due to a loose or disconnected driver (n=1), previous surgery/radiochemotherapy (n=2), tumor diameter < 2 cm (n=4). Finally, 15 patients (mean age: 50.20±9.03 years, range:35–65 years) were enrolled in this study cohort. According to pathological results, the patients were divided into three subgroups according to histological grade, FIGO stage, and myometrial invasiveness. MRE was performed on a 3.0T scanner (Discovery MR750; GE Healthcare, Waukesha, WI) with a pneumatic driver placed above the pelvis using a multislice, flow-compensated, spin-echo echo-planar imaging (SE-EPI), 3D-MRE sequence using 60-Hz vibrations (acquisition matrix: 80x80; TR/TE:1650/56.3 ms; single shot; FOV: 24 cm; number of slices: 20; slice thickness: 3 mm with 1-mm gap). The MRE magnitude and phase images were processed using a direct-inversion algorithm to calculate the stiffness. The ROIs excluded tumor edges, areas of significant wave interference and any other artifacts seen in the magnitude and wave images. The tumor ROI was drawn on the magnitude images with reference to conventional MR images. The Independent-Samples T-Test was used to compare the stiffness between different groups with a normal distribution. The Mann-Whitney U test was used to compare the stiffness between different groups with abnormal distributions. The diagnostic performance was determined with receiver operating characteristic (ROC) curve analysis. Statistical significance was defined as P<0.05.Results
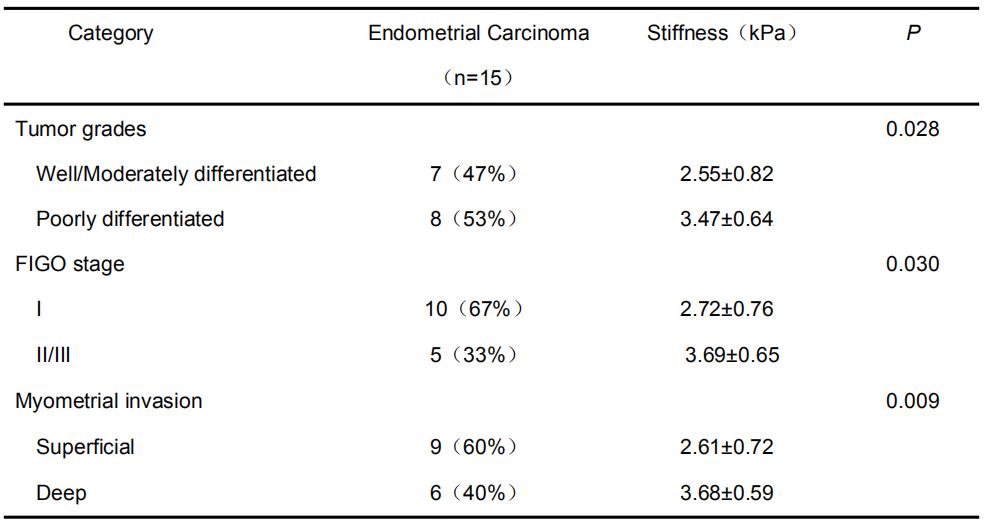
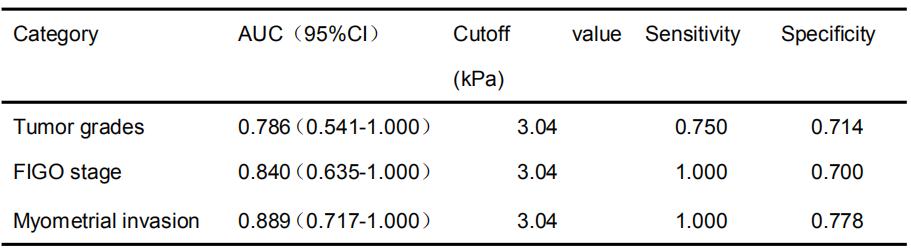
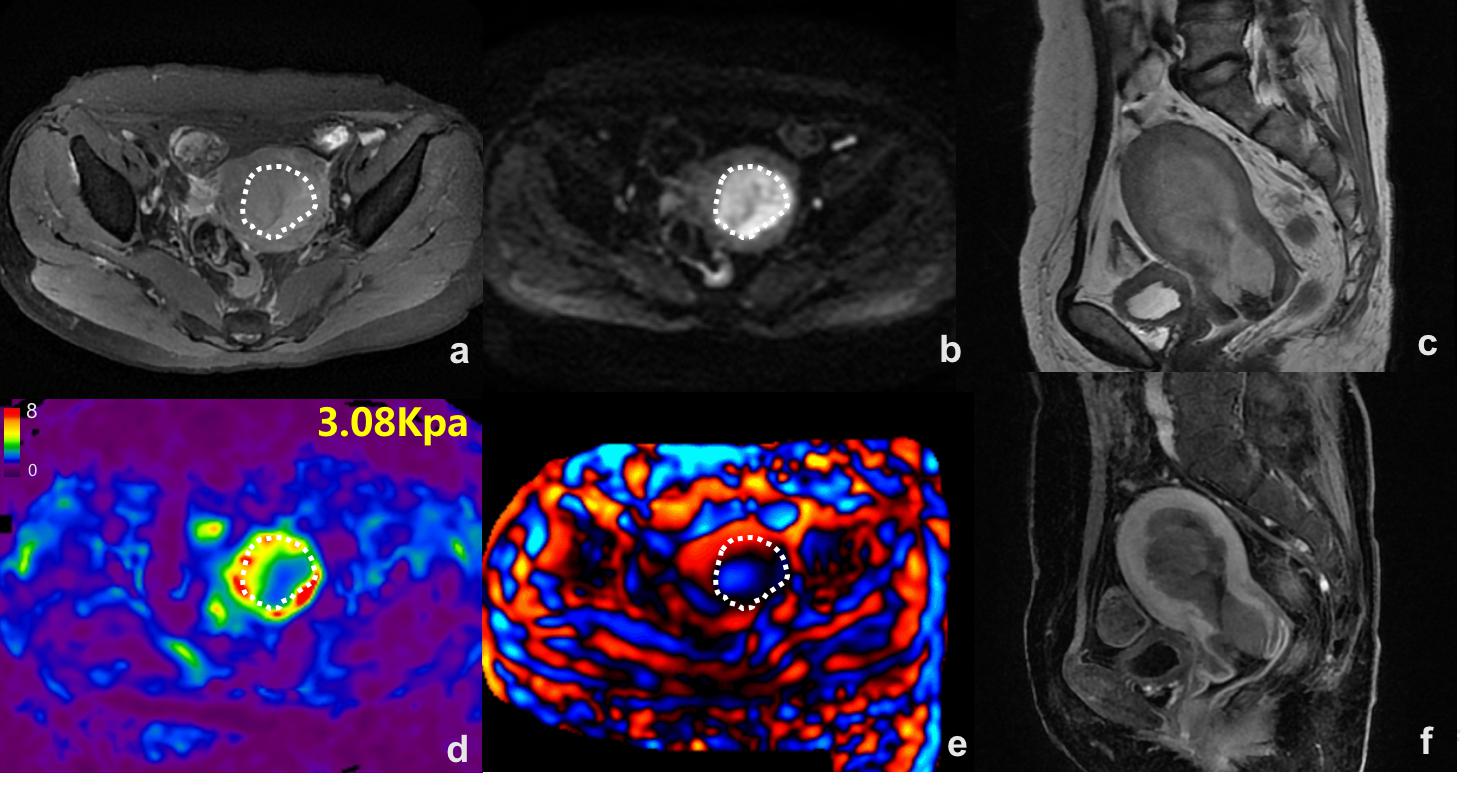
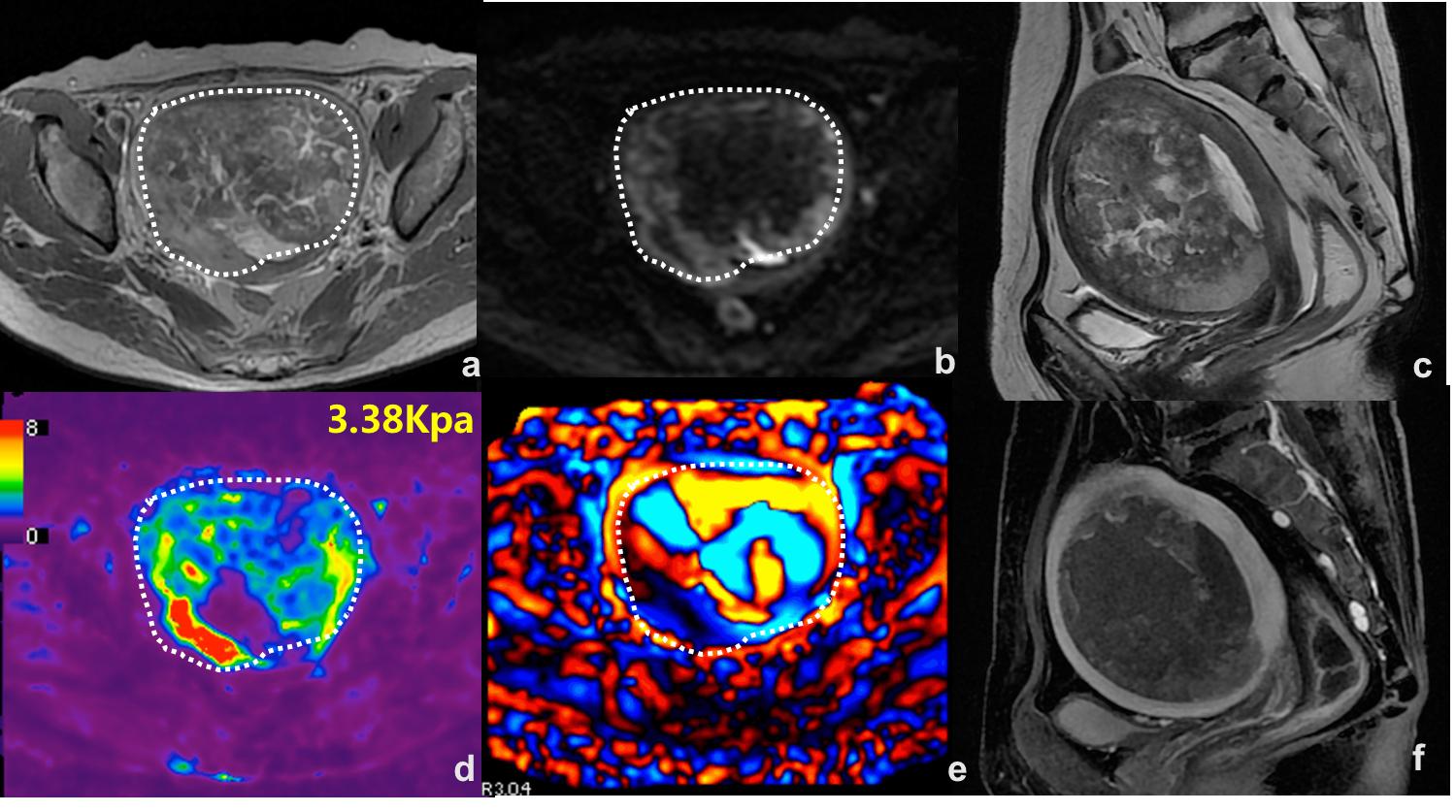
Pathological evaluation revealed 8/15 patients had pathologically confirmed, poorly differentiated EC; 7/15 had well or moderately differentiated EC. 10/15 patients were FIGO stage I EC, and 5/15 were FIGO stage II/III EC. 9/15 patients had pathologically confirmed deep myometrial invasiveness, and 6/15 had superficial myometrial invasion (Table 1). The stiffness of poorly differentiated EC was significantly higher than those that were well/moderately differentiated (3.47±0.64 kPa vs. 2.55±0.82 kPa, P =0.028). The area under the ROC curve was 0.786 (95% CI: 0.541-1.000, P=0.047). Using a stiffness of 3.04 kPa as a cutoff value resulted in 75% sensitivity and 71.4% specificity for differentiating poorly differentiated from well/moderately differentiated EC. The stiffness of FIGO stage II/III EC was significantly higher than that of FIGO stage I EC (3.69±0.65 kPa vs. 2.72±0.76 kPa, P=0.030). The area under the ROC curve was 0.840 (95% CI: 0.635-1.000, P=0.037). Using a stiffness of 3.04 kPa as a cutoff value resulted in 100% sensitivity and 70% specificity for differentiating FIGO stage I from FIGO stage II/III EC. The stiffness of EC with deep myometrial invasion was significantly higher than that with superficial myometrial invasion (3.68±0.59 kPa vs. 2.61±0.72 kPa, P=0.009). The area under the ROC curve was 0.889 (95% CI: 0.717-1.000, P=0.013). Using a stiffness of 3.04 kPa as a cutoff value resulted in 100% sensitivity and 77.8% specificity for differentiating deep myometrial invasion from superficial myometrial invasion of EC (Table 2) (Figures 1-3).Discussion
Our study showed that the stiffness of EC that were poorly differentiated, FIGO stage II/III, or had deep myometrial invasion was significantly higher than that of ones were well/moderately differentiated, FIGO stage I, or had superficial myometrial invasion, which is consistent with the results of a previous study with ultrasound elastography7,8. Our study also indicated that trans-pelvic 3D MRE could be useful as a potential method to improve EC diagnosis and treatment planning, Additional, larger patient studies are warranted to investigate its utility.Conclusion
In conclusion, tumor stiffness measured using 3D MRE may be potentially useful for assessing histological grade, FIGO stage and myometrial invasion of EC and may potentially aid in the preoperative risk stratification of EC.Acknowledgements
The authors state that this study has received funding by National Natural Science Foundation of China grant 81271562 (JW) and Science and Technology Program of Guangzhou, China 201704020016 (JW).References
1.Siegel RL, Miller KD, Jemal A. Cancer Statistics, 2017. CA Cancer J Clin. 2017;67(1):7-30.
2.Burke W M, Orr J, Leitao M, et al. Endometrial cancer: a review and current management strategies: part II. Gynecol Oncol,2014,134(2):393-402.
3.Chung HH, Kang SB, Cho JY, et al. Accuracy of MR imaging for the prediction of myometrial invasion of endometrial carcinoma. Gynecol Oncol. 2007;104(3):654-9.
4.Pepin K M, Ehman R L, Mcgee K P. Magnetic resonance elastography (MRE) in cancer: Technique, analysis, and applications. Prog Nucl Magn Reson Spectrosc,2015,90-91:32-48.
5.Thompson S M, Wang J, Chandan V S, et al. MR elastography of hepatocellular carcinoma: Correlation of tumor stiffness with histopathology features-Preliminary findings[J]. Magn Reson Imaging,2017,37:41-45.
6.Sinkus R, Siegmann K, Xydeas T, et al. MR elastography of breast lesions: understanding the solid/liquid duality can improve the specificity of contrast-enhanced MR mammography. Magn Reson Med. 2007;58(6):1135-44.
7.Nitta E, Kanenishi K, Itabashi N, et al. Real-time tissue elastography of uterine sarcoma. Archives of Gynecology and Obstetrics. 2014;289(2):463-5.
8.Preis K, Zielinska K, Swiatkowska-Freund M, et al. The role of elastography in the differential diagnosis of endometrial pathologies - preliminary report. Ginekologia Polska. 2011;82(7):494-7.
Figures