0092
4D Flow MRI Quantification of Congenital Shunts: Comparison to Invasive Catheterization1Cardiovascular Medicine, Univeristy of California San Diego, San Diego, CA, United States, 2Radiology, University of California San Diego, San Diego, CA, United States
Synopsis
When used for quantification of intracardiac and extracardiac shunts, 4D Flow MRI has been shown to have high reproducibility between measurement location and observers, and high consistency with MRI measurements of stroke volume. However, there has been little data showing its relationship to invasive measurements obtained during catheter angiography, which serves as the clinical reference standard at many institutions. We retrospectively evaluated patients who underwent 4D Flow MRI and invasive right heart catheterization during clinical work-up of congenital heart disease. 4D Flow measurements correlated extremely well with invasive measurements of shunt fraction by oximetry and cardiac output by Fick calculation in patients without a shunt.
Introduction
In patients with intracardiac and extracardiac shunts (atrial septal defects, ventricular septal defects, anomalous pulmonary venous return, and patent ductus arteriosus) determination of the severity of shunt is essential for surgical or interventional management. Invasive right heart catheterization with oximetry has been a long-standing reference standard for estimation of shunt fraction (1). Cardiac magnetic resonance imaging (MRI) with phase-contrast cine imaging has been shown to be reliable for quantifying shunt severity with fair correlation to invasive assessment (2). Recently, 4D Flow MRI has been shown to be more reliable for quantifying blood flow than conventional phase-contrast and enables quantification of multiple vessels without additional scan time (3,4,5). However, there has been little data directly comparing 4D Flow to invasive measurements. We thus hypothesized that 4D Flow would compare favorably to invasive measurements and sought to retrospectively assess this among patients who have undergone both exams.Methods
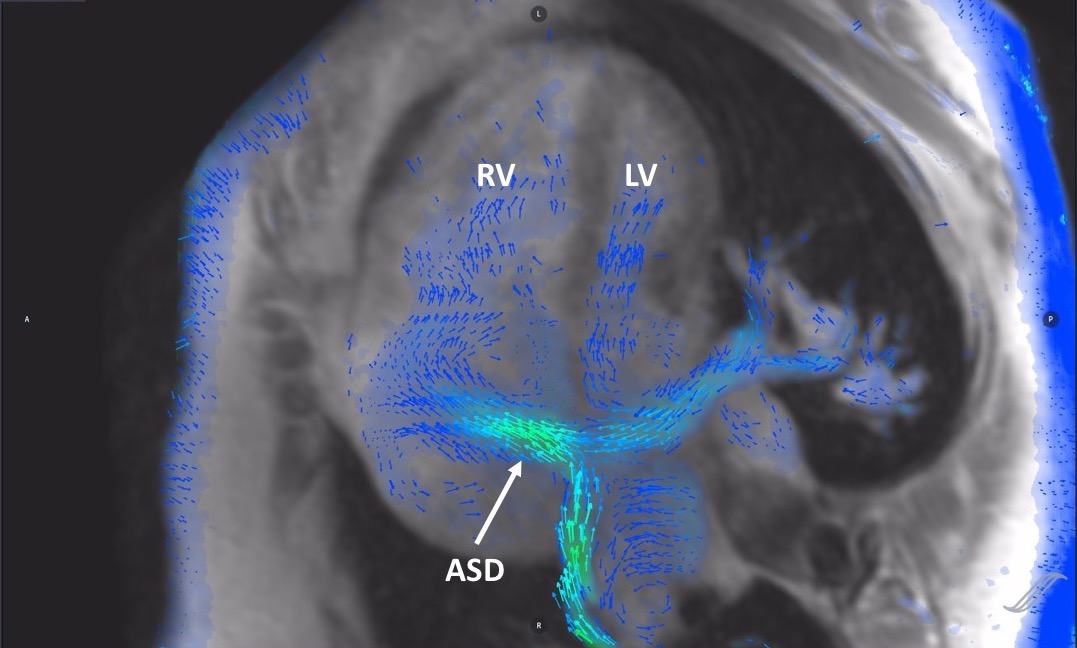
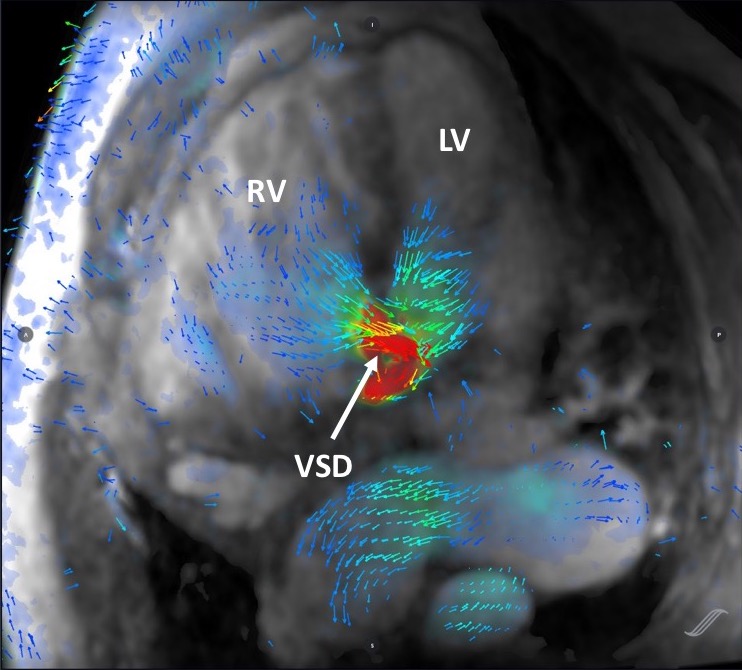
We performed a retrospective study including patients who underwent 3T MRI at our institution including post-contrast 4D Flow [figure 1,2,3] and cine SSFP ventricular volumetry, as well as invasive right heart catheterization with a shunt run. The study time frame included exams between August 2015 to November 2018. The time between MRI and catheterization had to be three months or less with no interval surgery or major change in clinical status between the studies. 4D Flow measurements were obtained using CardioAI v2.4 (Arterys, San Francisco, CA). The primary endpoint was comparison of estimated shunt fraction (QP/QS) by 4D flow and invasive assessment. Secondary end points included: (a) comparison of MRI-based RV/LV stroke volume ratio with catheterization, and (b) comparison of cardiac output between 4D flow and invasive catheterization using the Fick equation. Statistical analysis included Bland-Altman plots and Pearson correlation.Results
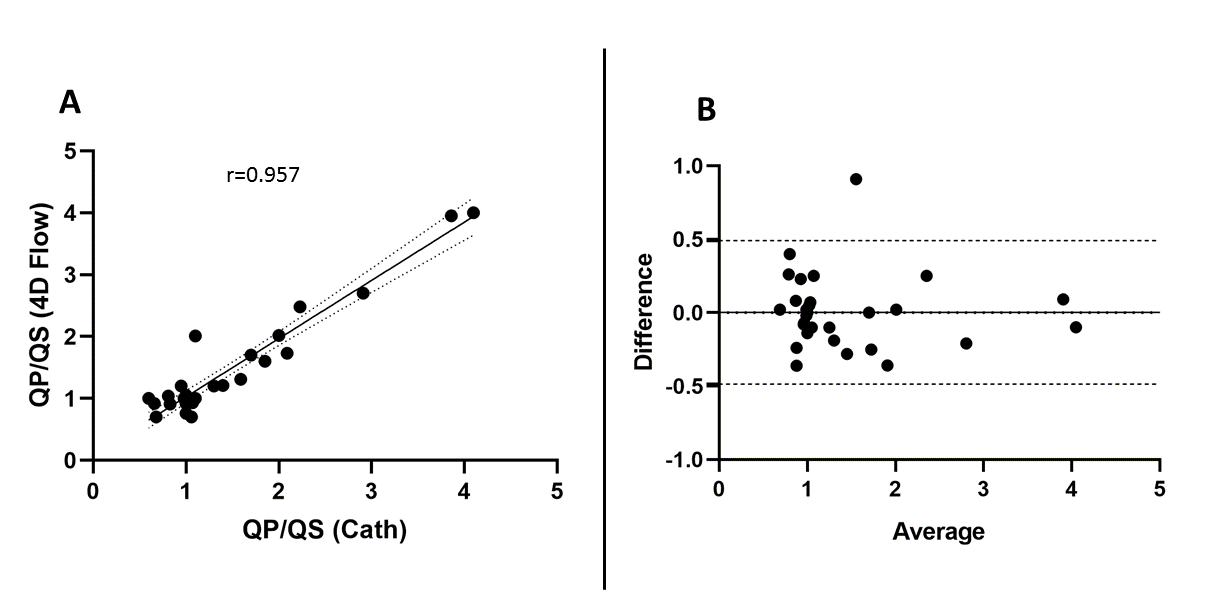
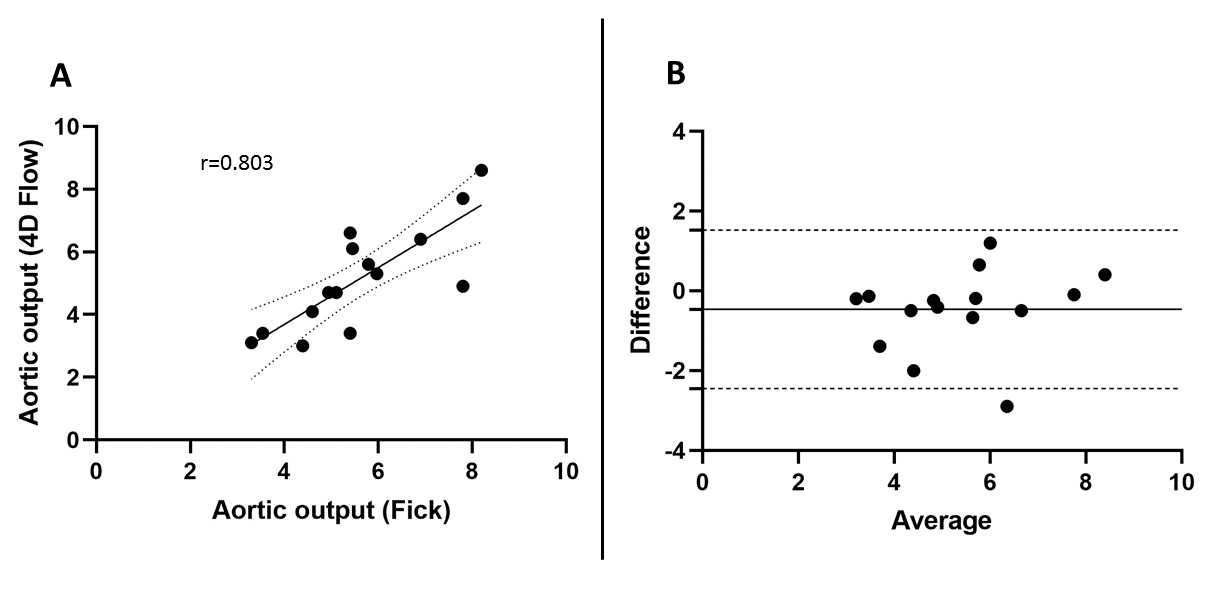
31 Patients were available for review who met inclusion criteria. Mean age was 49 years, 71% (n=22) were female, 11/31 (35%) had left to right shunt (QP/QS≥1.3), 5/31 (16%), had a right to left shunt (QP/QS<0.8), and 15/31 (48%), had no significant shunt (0.8≤QP/QS<1.3). Mean QP/QS by 4D Flow measurements and invasive catheterization was 1.415±0.86 and 1.417±0.843, respectively. 4D Flow QP/QS strongly correlated with catheterization (ρ=0.957) [figure 4]. There was no significant bias between 4D Flow and catheter-derived measurements of QP/QS(mean difference 0.003 L/min, limits of agreement -0.486 to 0.491 L/min). RVSV/LVSV correlated well with 4D Flow QP/QS (ρ=0.835) but did not correlate as strongly to catheterization (ρ=0.784), acknowledging that the use of RVSV/LVSV ratio to estimate shunt fraction may be compromised by concomitant valvular regurgitation. Including all patients, Fick-derived cardiac output did not correlate well with 4D flow measurements (ρ=0.361). However, in the 15 patients who had CO measurements by Fick with no shunt, there was good correlation with 4D Flow (ρ=0.803) [figure 5]. 4D Flow slightly underestimated cardiac output relative to Fick (mean difference 0.466 L/min).Discussion
We demonstrate in this study the relationship between 4D Flow MRI and invasive measures of shunt fraction and cardiac output via cardiac catheterization. We demonstrate that shunt calculation by 4D flow compares well to invasive assessment with excellent correlation between the two modalities. Cardiac output by Fick equation correlated poorly, likely due to a confounding effect when a shunt is present. In patients without a shunt, correlation of cardiac output between catheterization and 4D Flow improved.Acknowledgements
No acknowledgement found.References
1. Antman EM, Marsh JD, Green LH, Grossman W. Blood oxygen measurements in the assessment of intracardiac left to right shunts: a critical appraisal of methodology. Am J Cardiol 1980;46:265–71
2. Debl K, Djavidani B, Buchner S,. The British Journal of Radiology 2009 82:977, 386-391
3. Hsiao A, Alley MT, Massaband P, Herfkens RJ, Chan FP, Vasanawala SS. Improved cardiovascular flow quantification with time‐resolved volumetric phase‐contrast MRI. Pediatr Radiol 2011;41:711–720
4. Hsiao, A., Yousaf, U., Alley, M. T., Lustig, M., Chan, F. P., Newman, B., & Vasanawala, S. S. (2015). Improved quantification and mapping of anomalous pulmonary venous flow with four-dimensional phase-contrast MRI and interactive streamline rendering. Journal of Magnetic Resonance Imaging, 42(6), 1765–1776. https://doi.org/10.1002/jmri.24928
5. Chelu, R. G., Horowitz, M., Sucha, D., Kardys, I., Ingremeau, D., Vasanawala, S., … Hsiao, A. (2018). Evaluation of atrial septal defects with 4D flow MRI—multilevel and inter-reader reproducibility for quantification of shunt severity. Magnetic Resonance Materials in Physics, Biology and Medicine. https://doi.org/10.1007/s10334-018-0702-z
Figures