0091
Chronological 4D Flow MRI Assessment of Pulmonary Artery Stenosis Stent Treatment1Biomedical Engineering, University of Wisconsin - Madison, Madison, WI, United States, 2Mechanical Engineering, University of Wisconsin - Madison, Madison, WI, United States, 3Pediatrics, University of Wisconsin - Madison, Madison, WI, United States, 4Radiology, University of Wisconsin - Madison, Madison, WI, United States
Synopsis
Branch pulmonary artery stenosis, a common complication after surgical repair of congenital heart disease, is treated with intravascular stenting. As the acute and chronic effects of stenting are unknown this study uses 4D Flow MRI to serially monitor hemodynamics in a porcine model of pulmonary artery stenosis. Intervention increases flow through the stenosed artery, but not to a normal value. Chronologically, stenosis flow is found to increase immediately after stenting and then remain constant.
Introduction
Certain complex forms of congenital heart disease (CHD) require surgical repair during infancy1. A commonly encountered post-operative complication of these early surgeries is branch pulmonary artery stenosis (PAS)2-6 which is associated with both acute and chronic morbidity and mortality7-10. Catheter interventions with intravascular stenting are a first line therapy for post-surgical PAS in older patients and with technological advances this therapy is now being utilized in infants and small children. Little is known about the acute and chronic consequences of stent therapy for treatment of post-surgical PAS occurring early in life. This project uses serial 4D Flow MRI to define the hemodynamic consequences of early stent interventions with serial dilations in a porcine PAS model.Methods
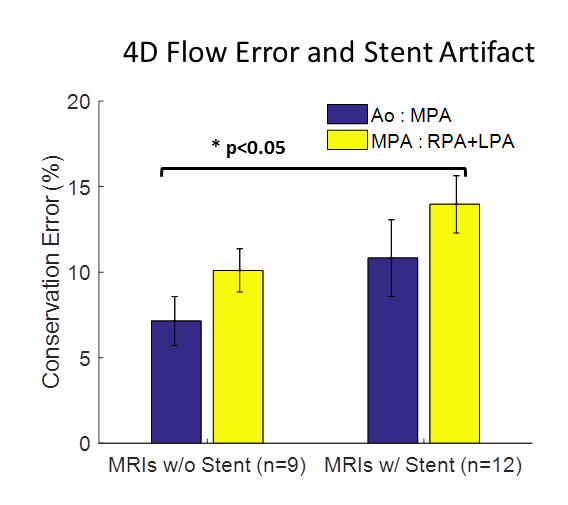
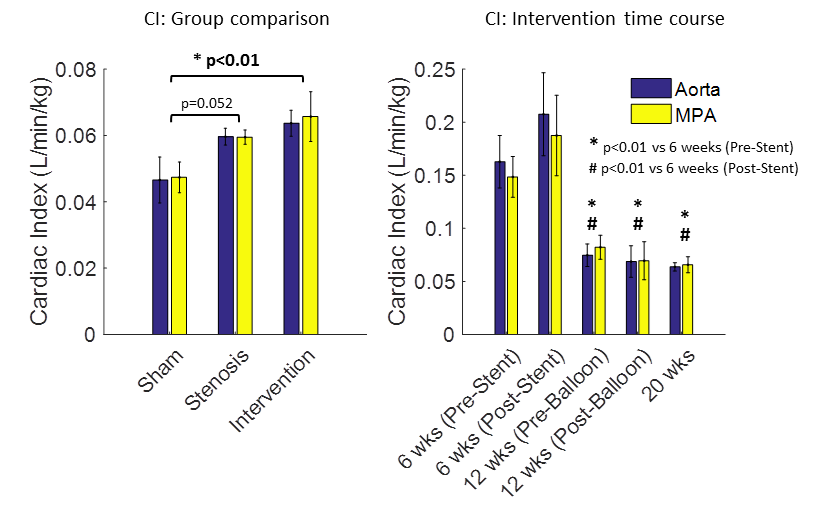
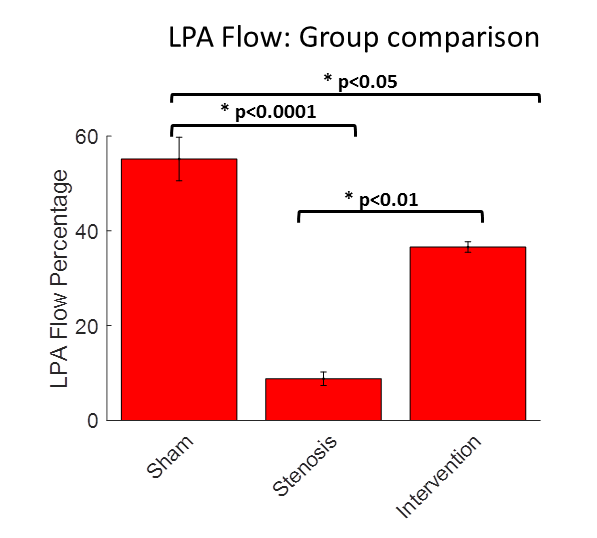
Isolated left PAS was created in neonatal piglets (n=3, 5. 4 kg) by suturing a short segment of Gore-Tex tube graft around the proximal left PA (LPA). Cardiac catheterizations with pre and post intervention MRI occur at 6, 12 and 20 weeks of age (56 Kg) for intervention animals. Sham (n=3) and stenosis control (n=3) animals only have imaging and catheterization at 20 weeks of age. LPA stenting occurred at 6 weeks then LPA stent dilation at 12 weeks. No intervention was performed at 20 weeks. MRI is performed on a 3. 0T scanner using the 4D Flow MRI sequence PC-VIPR (Phase Contrast Vastly Under sampled Projection Imaging)11,12. 4D Flow MRI quantitatively and qualitatively assesses cardiac and vascular blood flow. Analysis planes and streamlines are shown in Fig1. Internal consistency of the 4D Flow MRI data for MRIs with and without stents was evaluated following conservation of mass principles as the percent difference in flow rates (aorta:PA and PA:LPA+RPA). Cardiac index (CI) is cardiac output (CO) normalized by body weight. LPA flow percentage is an important metric for the success of PAS stenting and is calculated as LPA flow divided by CO measured in the PA. Statistical analysis is performed using ANOVA with post hoc hypothesis testing using the Bonferroni correction for multiple comparisons.Results
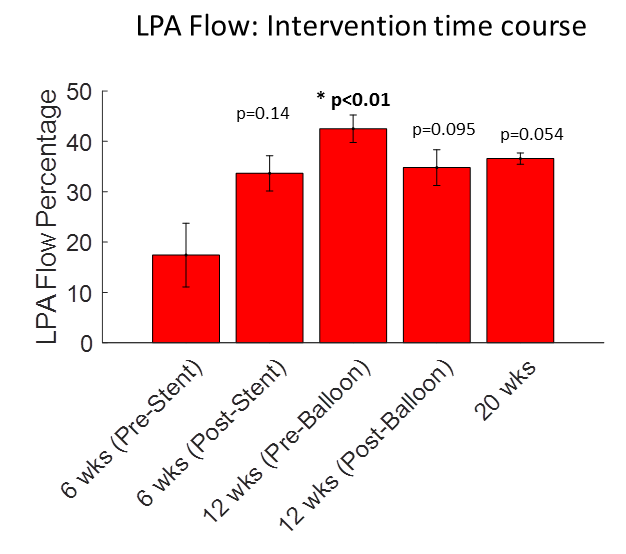
Mass conservation error exhibits a trend of being greater in MRIs with a stent compared to MRIs without a stent (Fig2). The PA:LPA+RPA conservation error with a stent is greater than the aorta:PA mass conservation error without a stent . At 20 weeks, CI is greater in the intervention than sham group (Fig3). In intervention animals, CI does not change acutely for stenting or balloon dilation but decreases over time. LPA flow percentage is decreased in the stenosis group (Fig4). Intervention increases LPA flow percentage from 9% to 37%, but not to the level of the sham group. Pre-stenting only 17% of flow goes to the LPA while at 20 weeks 37% of flow is to the LPA (Fig3). LPA flow percentage increases after stenting and not balloon dilation (Fig5) suggesting the initial stenting is responsible for most of the therapeutic benefit.Discussion
The finding that PAS stenting increases LPA flow percentage is a significant finding for PAS treatment. A previous study with this animal model found that PAS impaired vascular development, measured by the diameter of LPA branch vessel diameters, and that intervention resulted in a comparable level of vascular development to the sham group13. Improved but still impaired LPA flow with normal vascular development is a promising finding, as LPA flow would not need to be improved to healthy values to have normal vascular growth. Differences in CI between the three groups are unexpected as a previous PAS study found no differences in CI measured with thermodilution13. Chronologically, LPA flow increases after stenting then does not change after balloon dilation. Currently only the 12 weeks pre-ballooning time point is significantly different from the 6 weeks pre-stent time point, however the study is ongoing and when fully powered we expect several of these time points to reach statistical significance.
More broadly, this study demonstrates the capability of 4D-flow MR to comprehensively examine the acute and chronic effects of minimally invasive interventions. While MRI signal is lost due to the stent, flow is still able to be quantified proximal and distal to the stent. For chronological studies looking at the time course of an intervention, 4D flow is non-invasive unlike heart catheterization and provides greater information than other non-invasive modalities like ultrasound.
Conclusion
4D flow MRI measured pulmonary flow distribution is improved after PAS stenting compared to stenosis control but is impaired relative to sham. LPA flow increases after the initial stenting then remains relatively constant over the remainder of the study. Future work will include additional PA stenting animals (n=10 total) compared to sham and untreated stenosis controls and analyze ventricle function using 4D flow metrics of kinetic energy and vorticity.Acknowledgements
This investigation was supported by the National Institutes of Health, under Ruth L. Kirschstein National Research Service Award T32 HL 007936 from the National Heart Lung and Blood Institute to the University of Wisconsin-Madison Cardiovascular Research Center. The project described was also supported by the Clinical and Translational Science Award (CTSA) program, through the NIH National Center for Advancing Translational Sciences (NCATS), grant UL1TR000427. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.References
1. Hoffman J, Christianson R. Congenital heart disease in a cohort of 19,502 births: long term follow up. Am J Cardiol 1978;42:641-47.
2. Hirsch J, Mosca R, Bove E. Complete Repair of Tetraology of Fallot in the Neonate. AnnSurg 2000;232:508-14.
3. Parry A, McElhinney D, Kung G, Reddy V, Brook M, Hanley F. Elective primary repair of acyanotic tetralogy of Fallot in early infancy: overall outcome and impact on the pulmonary valve. J Am Coll Cardiol 2000;36:2279-83.
4. Groh M, Meliones J, Bove E, et al. Repair of tetralogy of Fallot in infancy. Effect of pulmonary artery size on outcome. Circulation 1991;84:III206-12.
5. Kim H, Sung S, Chang Y, Lee H, Park J. Early and midterm outcomes of left pulmonary artery angioplasty using anterior wall flap of the main pulmonary artery in tetralogy of Fallot repair. J Thorac Cardiovasc Surg 2014;148:2597-601.
6. Wilder T, Van Arsdell G, Pham-Hung E, et al. Aggressive Patch Augmentation May Reduce Growth Potential of Hypoplastic Branch Pulmonary Arteries After Tetralogy of Fallot Repair. Ann Thorac Surg 2016;101:996-1004.
7. Gatzoulis M, Balaji S, Webber S, Siu S, et al. Risk factors for arrhythmia and sudden death late after repair of tetralogy of Fallot: a multicenter study. Lancet;356:975-81.
8. Harrison D, Harris L, Sui S, MacLoghlin C, et al. Sustained ventricular tachycardia in adult patients late after repair oftetralogy of Fallot. J Am Coll Cardiol. 1997;30:1368-73.
9. Rhodes J, Dave A, Pulling M, Geggel R, et al. Effect of pulmonary artery stenosis on the cardiopulmonary response to exercise following repair of tetralogy of Fallot. Am J Cardiol. 1998;81:1217-9.
10. Giardini A, Khambadkone S, Rizzo N, Riley G, et al. Determinants of Exercise Capacity After Arterial Switch Operation for Transposition of the Great Arteries. Am J Cardiol 2009;104:1007-1012.
11. Wieben O, Francois C, Reeder S, Cardiac MRI of ischemicheart disease at 3 T: potential and challenges. Eur J Radiol, 2008. 65(1):15-28.
12. Francois, C, et al., 4D cardiovascular magnetic resonance velocity mapping of alterations of right heart flow patterns and main pulmonary artery hemodynamics in tetralogy of Fallot. J Cardiovasc Magn Reson 2012(14):16-22.
13. Bates, M, et al., Consequences of an early catheter‐based intervention on pulmonary artery growth and right ventricular myocardial function in a pig model of pulmonary artery stenosis, Catheterization and Cardiovasc Intervention 2018. 92(1):78-87
Figures