0081
In vivo magnetic resonance imaging demonstrates that subcutaneous administration angiotensin-(1-7) is neuroprotective following severe traumatic brain injury in mice1Pharmacology and Molecular Therapeutics, Program in Molecular and Cell Biology, Uniformed Services University, Bethesda, MD, United States, 2Radiology and Radiological Sciences, Uniformed Services University, Bethesda, MD, United States, 3Center for Neuroscience and Regenerative Medicine, Henry M. Jackson Foundation, Bethesda, MD, United States, 4Center for Neuroscience and Regenerative Medicine, Uniformed Services University, Bethesda, MD, United States
Synopsis
The effectiveness of angiotensin-(1-7), a novel peptide derivative of angiotensin II, for the treatment of traumatic brain injury in mice have been investigated using non-invasive MRI techniques. Our results demonstrate that treatment of mice with angiotensin-(1-7) after control cortical impact reduced lesion volume compared to saline-treated mice. The MRI data are validated by histological results. The observed data show for the first time that angiotensin-(1-7) has potential therapeutic use for TBI.
Introduction
Traumatic brain injury (TBI) frequently leads to long-term cognitive problems and physical disability with no effective therapieis. The octapeptide angiotensin II (Ang II), acting as a ligand at the angiotensin II type 1 receptor (AT1R), plays an important role in the regulation of blood pressure. Treatment with the angiotensin receptor blockers (ARBs) candesartan or telmisartan reduce inflammation, improve cerebral blood flow, reduce the lesion volume, and enhance spatial memory up to a month after injury1. Further, AT1R knockout mice showed less glial activation and reduced lesion volume after control cortical impact (CCI) injury in comparison to wild type mice. These suggest that Ang II acting through the AT1R is detrimental to recovery from TBI in mice.
Although Ang II was thought to be the primary effector of the renin angiotensin system (RAS), a novel peptide derivative of Ang II, angiotensin-(1-7) (Ang-(1-7)), was discovered and shown to act largely in opposition to Ang II. The endocarboxypeptidase angiotensin converting enzyme 2 (ACE2) cleaves the terminal phenylalanine of Ang II to produce Ang-(1-7), changing its receptor specificity. Ang-(1-7) signals through the G-protein coupled Mas receptor. This alternate ACE2/Ang-(1-7)/Mas receptor axis of the RAS acts to counter Ang II signaling at many levels, and has anti-inflammatory, vasodilatory, and neuroprotective effects of its own2-5. Previously we showed that pharmacologic blockade of AT1R had efficacy in improving recovery from CCI injury in the mouse. The goal of this study was to utilize both in vivo MRI and histology to determine whether administration of Ang-(1-7) would also be beneficial in this TBI model.
Methods
C57BL/6 mice were injured by CCI at 8-10 weeks. Sham animals underwent anesthesia and scalp incision without a craniectomy or injury. In the initial experiment, Ang-(1-7) (1mg/kg) or vehicle (saline) was administered daily by subcutaneous injection, beginning 1 hour post injury (hpi), until animals were sacrificed at 3 days post injury (dpi). In the second experiment, mice were injured identically, Ang-(1-7) (1mg/kg) or vehicle treatment was started by subcutaneous injection at 6 hpi, and an osmotic minipump was implanted subcutaneously at 24 hpi where it continuously administered Ang-(1-7) (1mg/kg/day) or vehicle until the mice were sacrificed at 29 dpi. Lesion volume was assessed using histological methods and T2-weighted MRI and computed T2 maps. Microgliosis, astrogliosis, capillary density, and neuronal loss at 3 and 29 dpi were assessed using immunohistochemical staining against IBA-1, GFAP, CD31, and NeuN, respectively.
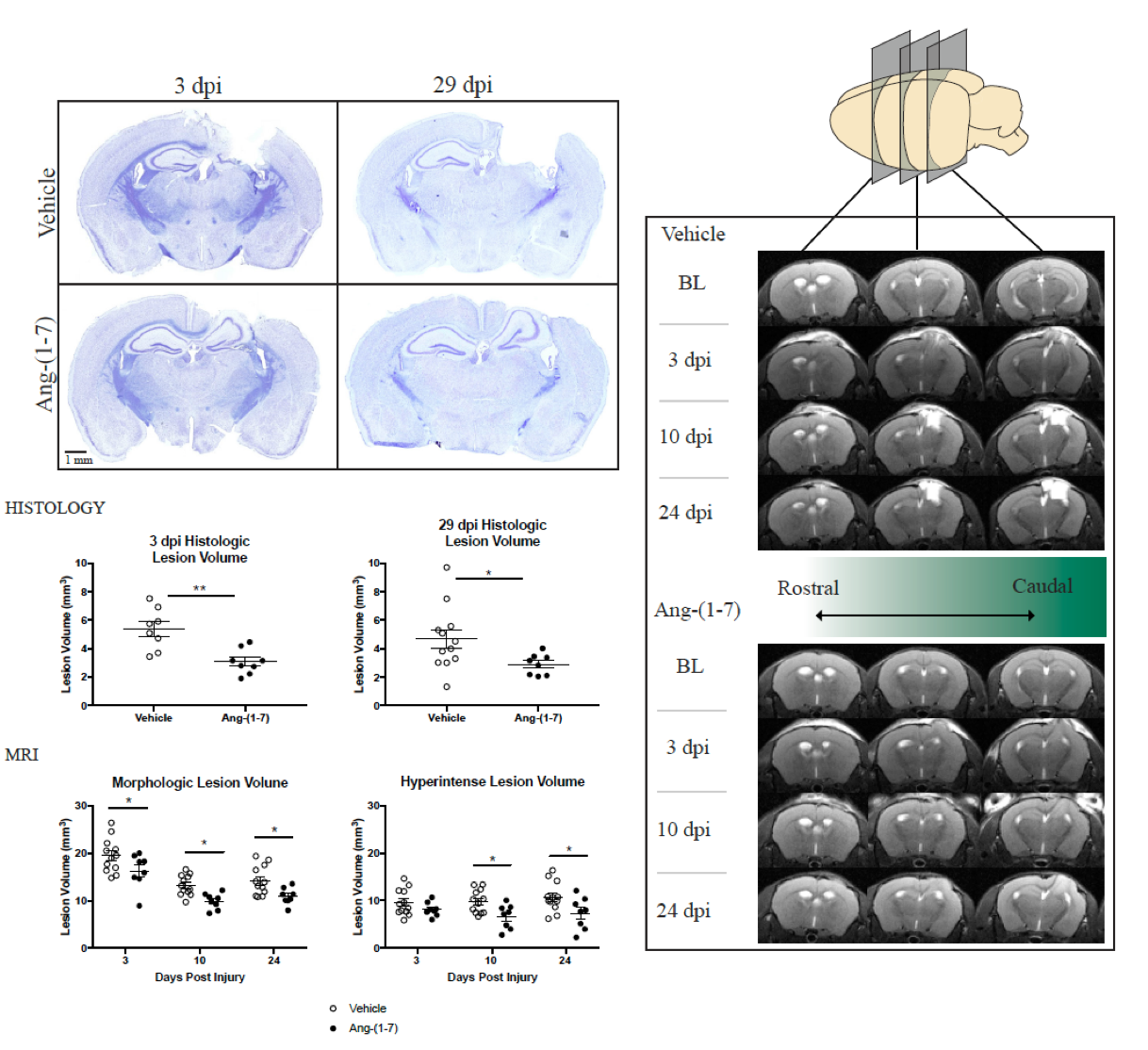
MRI experiments were conducted using a 7T Bruker Biospec 70/20 (Bruker Biospin, Billerica, MA). Each mouse underwent MRI 7 days prior to injury, and 3, 10 and 24 dpi. The PDW/T2W/T2maps were acquired using multi echo 2D Rapid Acquisition with Relaxation Enhancement with the following parameters: repetition time 4500 ms, echo time 10, 30, 50, 70, 90, 110 ms, echo train length 2, number of averages 4, field of view 13.8x11.2 mm2, in-plane resolution 150x150 μm2, slice thickness 600 μm. Lesion was defined under two predetermined classifications: morphologic lesion (visual morphologic difference between normal and abnormal brain structures) and hyper-intense lesion (volume derived base on T2 values deviated more than 2 standard deviation from normal values within morphologic lesion). All quantification was performed using VivoQuant (InVicro, Boston, MA) software by a blinded investigator. The quantitative results were evaluated using two-away ANOVA with Sidak’s multiple comparison test. All statistics were performed via Prism 7 software (GraphPad).
Results and Discussion
Ang-(1-7) treatment prevented significant motor deficits from developing at 3 dpi and significantly attenuated injury-induced memory deficits at 28 dpi. Measurement of lesion volume by cresyl violet histology revealed a significant volume reduction of the CCI-induced cortical-hippocampal cavity at both three and 29 dpi in Ang-(1-7) treated mice when compared to treatment with vehicle. MRI independently revealed that Ang-(1-7) significantly reduced lesion volume calculated by different criteria (morphological versus hyperintense) at various time points (Figure 1). Microgliosis, but not astrogliosis, was significantly reduced at 3 dpi in Ang-(1-7) treated mice. Ang-(1-7) significantly reduced astrogliosis, and some microgliosis, at 29 dpi. Neuronal and capillary loss was significantly decreased at 29 dpi after Ang-(1-7) treatment.Summary
Our results revealed that subcutaneous administration of Ang-(1-7), following CCI in mice, acutely and chronically reduced lesion volume when measured by MRI or histology. In addition, Ang-(1-7) prevented chronic capillary and neuronal loss, reduced microgliosis and astrogliosis, and ameliorated motor function and memory deficits associated with CCI. Overall, this study confirms that the Ang-(1-7) robustly attenuated various pathological features of traumatic brain injury in a rodent model. Moreover, these data show for the first time that Ang-(1-7) has potential therapeutic use for TBI.Acknowledgements
This work was funded by the U.S. DOD in the Center for Neuroscience and Regenerative Medicine.References
- Villapol, Sonia, et al. “Neurorestoration after Traumatic Brain Injury through Angiotensin II Receptor Blockage.” Brain, vol. 138, no. 11, 2015, pp. 3299–3315.
- Xu, Ping, et al. “ACE2/ANG-(1-7)/Mas Pathway in the Brain: the Axis of Good.” American Journal of Physiology-Regulatory, Integrative and Comparative Physiology, vol. 300, no. 4, 2011.
- Sumners, Colin, et al. “Protective Arms of the Renin-Angiotensin-System in Neurological Disease.” Clinical and Experimental Pharmacology and Physiology, vol. 40, no. 8, 2013, pp. 580–588.
- Mecca, Adam P., et al. “Cerebroprotection by Angiotensin-(1-7) in Endothelin-1-Induced Ischaemic Stroke.” Experimental Physiology, vol. 96, no. 10, 2011, pp. 1084–1096.
- Bennion, Douglas M., et al. “Neuroprotective Mechanisms of the ACE2/Angiotensin-(1-7)/Mas Axis in Stroke.” Current Hypertension Reports, vol. 17, no. 2, 2015.
Figures