0077
Connectivity Reorganization after Repetitive Mild Traumatic Brain Injury is Impact Site Associated1Neuroscience Research Center, Taipei Medical University, Taipei, Taiwan, 2Department of Radiology, School of Medicine, College of Medicine, Taipei Medical University, Taipei, Taiwan, 3Translational Imaging Research Center, Taipei Medical University Hospital, Taipei, Taiwan, 4Department of Biomedical Imaging and Radiological Sciences, National Yang-Ming University, Taipei, Taiwan, 5Department of Biomedical Imaging and Radiological Science, China Medical University, Taichung, Taiwan, 6Department of Medical Imaging, Taipei Medical University Hospital, Taipei, Taiwan
Synopsis
Different degrees of functional reorganization associated with
Introduction
The concerns of repetitive mild traumatic brain injury (rmTBI) are increasingly recognized.1 Brain vulnerability likely increases after the first mTBI, and subsequent insults may exacerbate the injury outcomes. The latest findings from the largest donated brain cohort from football players suggested that different football-related factors primarily varied based on individual playing positions, such as the number and frequency of concussions, the frequent location of head impact, the self-reported concussion incidence2, 3, may be correlated to the risk of chronic traumatic encephalopathy (CTE).4 Nevertheless, the wide spectrum of impact parameters from the recruited clinical cases complicates outcome prediction and also hinders the development of therapeutic strategy of mTBI. Specifically, how the impact site, which was presumed to augment the initial neuroinflammatory cascade, to govern the subsequent recovery mechanisms and to prime the tissue for chronic inflammation5, may alter the susceptibility of the brain to subsequent injury remains unclear. Herein, rather than using the animal models with acute focal brain contusion or hemorrhage, we perform repetitive close-head injury (CHI) in rats to mimic rmTBI6 and monitor the change of functional connectivity after CHI targeting different brain regions. Our finding shows the different connectivity patterns as impact sites changed, implying the change of brain connectivity may be used to retrospectively explore the impact site of rmTBI without significant structural damage.Methods
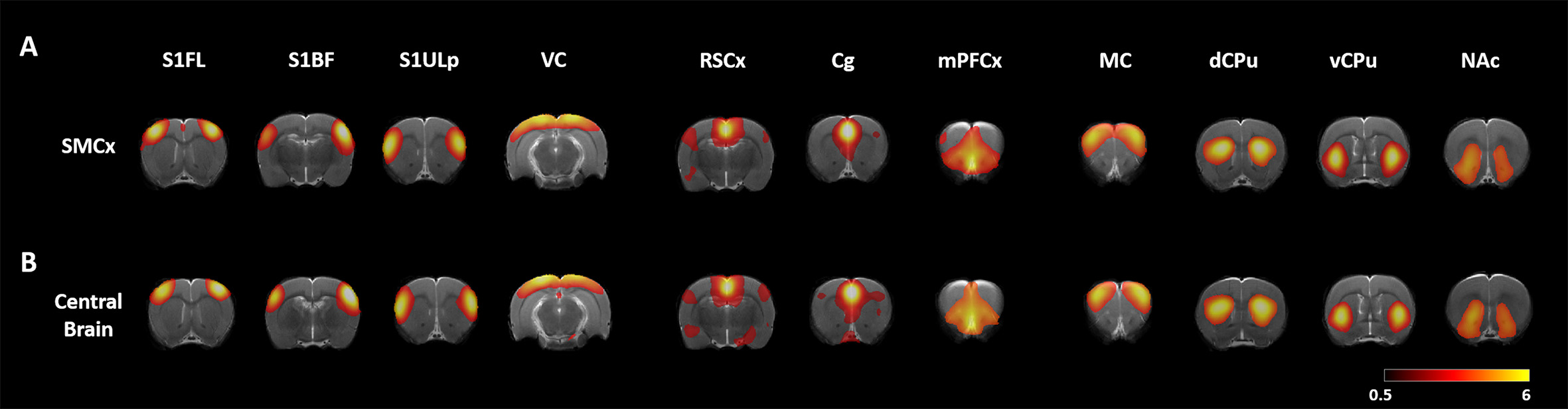
Male Sprague–Dawley rats were anesthetized with Chloral Hydrate for two CHI injury within 1 h targeting on the skull on top of the left sensorymotor cortex (SMCx, n=10) or the center skull in between the bregma and lambda (Central Brain, n=10). Longitudinal MRI was performed pre, at 24 h, and day 50 after CHI. Animals were anesthetized under the cocktail protocol with dexmedetomidine and isoflurane for MRI on a Bruker 7 T PharmaScan.7, 8 rsfMRI was acquired using the single-shot echo-planar imaging (EPI) with TR/TE= 1000/15 ms, FOV= 3.5 ×3.5 cm, matrix size = 64×64, 16 slices, slice thickness of 1 mm and number of repetition= 300 for total scan time= 5 min. T2-weighted images with the same geometry were also acquired. Slice timing and spatial smoothing were performed on SPM8 after pre-processing. rsfMRI data were analyzed using gICA with 25 components by GIFT. Major functional connectivity map of our interest networks including sensory, default mode network (DMN) and motor was extracted (Fig 1). Statistical analysis between different time points was conducted using dual-regression approach. Pearson correlation coefficient was calculated and presented after Z transformation.7, 8 One-sample t-test was employed to determine the significance of functional connectivity within a condition (p<0.05, with FDR correction). Two-sample t-test was used to determine the differences between pre- and post-rmTBI, and between impact sites (p<0.05).Results & Discussion
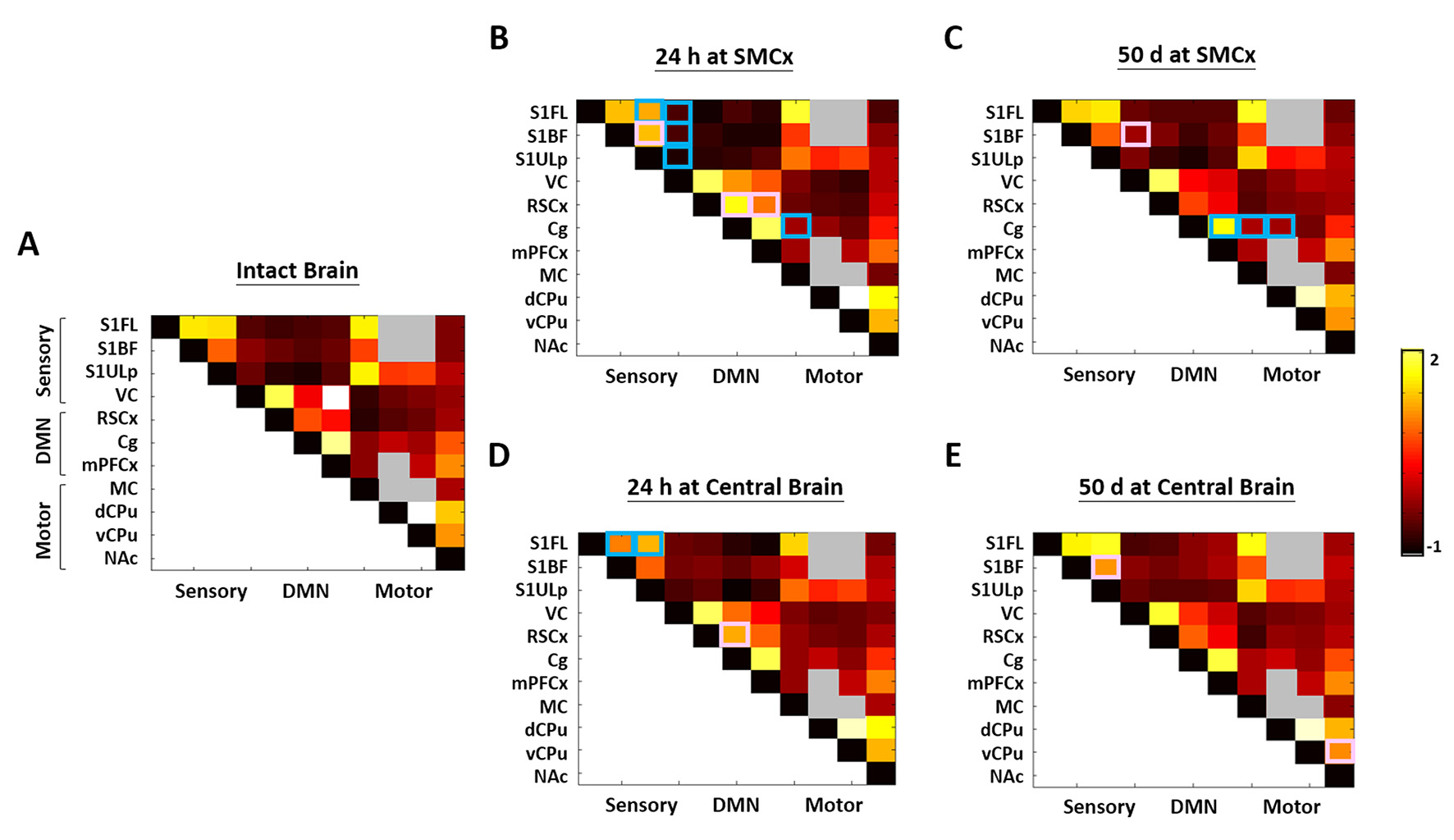
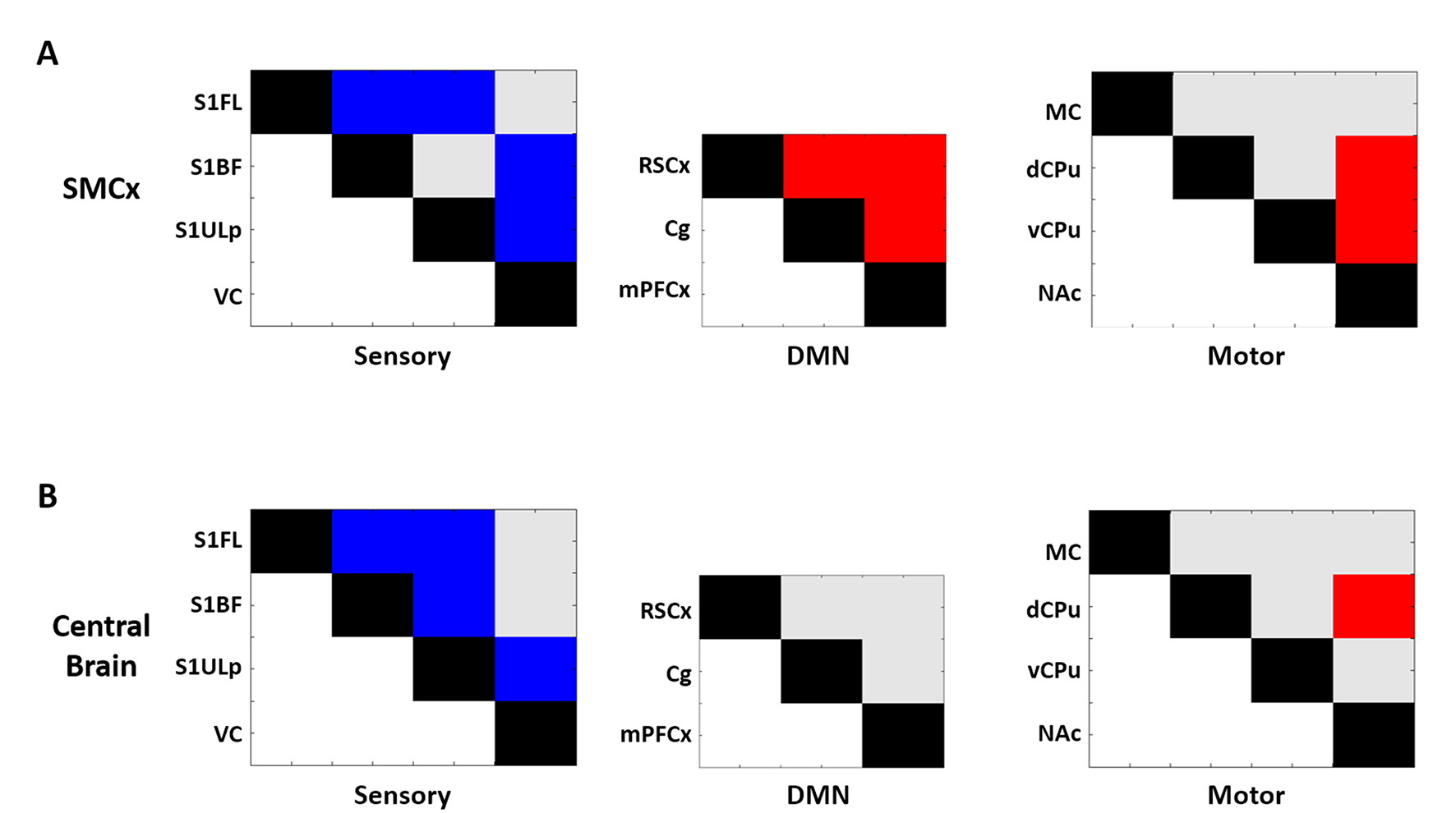
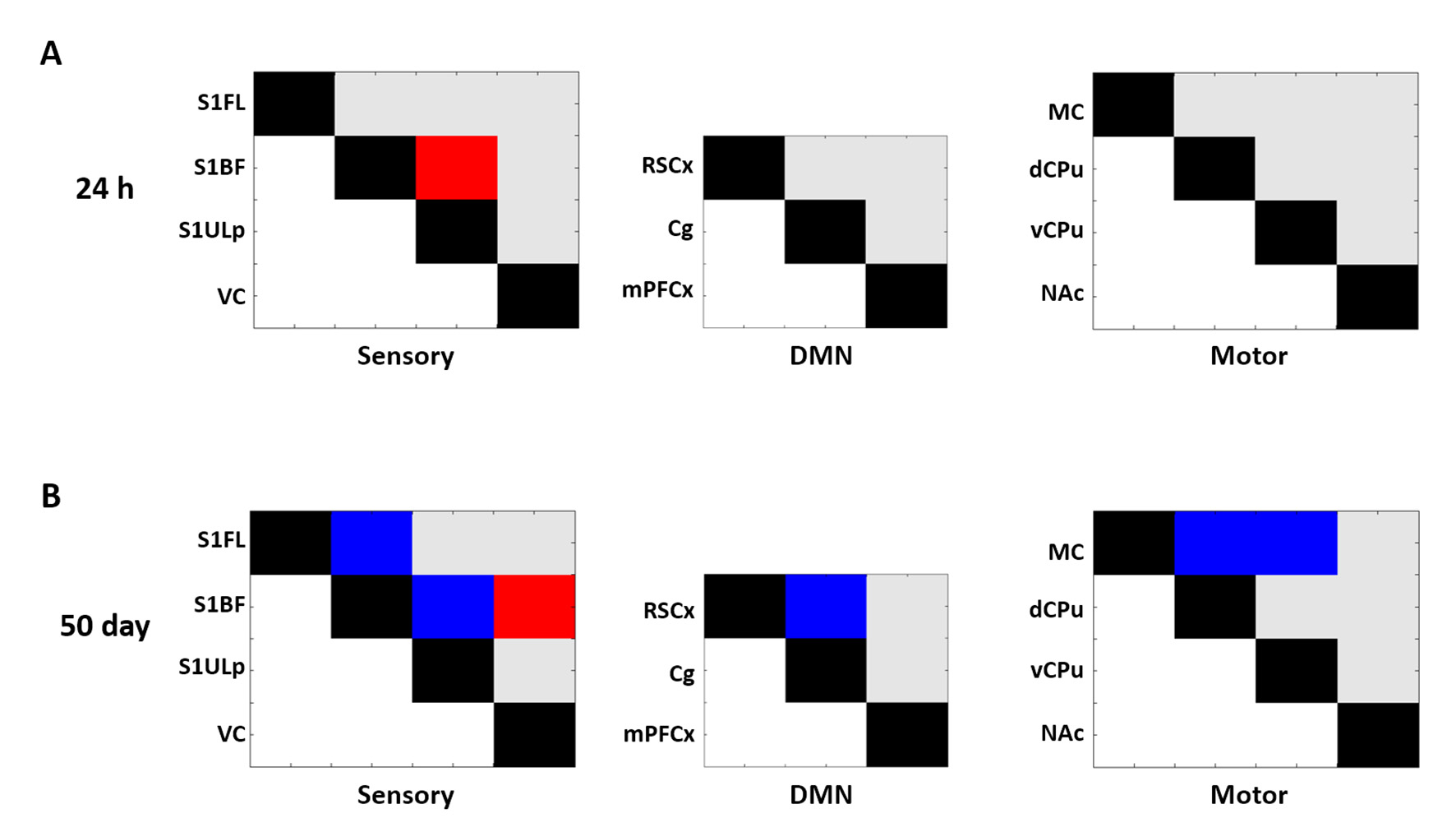
Regardless of the impact sites, major functional regions in the interested networks were preserved after rmTBI (Fig 1) as no significant macroscopic damage to the brain after CHI.6 Nevertheless, our connectivity analysis revealed functional reorganization after injury compared with the intact brains (Fig 2). At 24h h after SMCx rmTBI, significant decrease of connectivity was observed in most of sensory regions; significant increase of connectivity was observed between RSCx and two other DMN regions (Fig 2B). At 24 h after central brain rmTBI, significant decrease of connectivity was observed between S1FL and other somoatosensory regions (S1BF and S1ULp); significant increase of connectivity was observed between RSCx and Cg (Fig 2D). Compared with the connectivity at 50 days, most of sensory regions showed lower connectivity regardless of impact sites (Fig 3A&B). However, significant stronger connectivity was observed in DMN and between NAc and CPu regions after SMCx rmTBI (Fig 3A). The results may suggest the wider reorganization after the unilateral rmTBI. Compared with central brain rmTBI, significant higher connectivity between S1BF and S1ULp was observed at 24h after SMCx rmTBI (Fig 4A). In contrast, lower connectivity was found in multiple regions at 50 days after SMCx rmTBI (Fig 4B). Together with significant connectivity change between 24 h and 50 days (Fig 3A), SMCx rmTBI may induce long-lasting in functional reorgnaization compared with central brain rmTBI. Our results demonstrated that even without significant structural damage, the impact site of rmTBI may affect the functional organization after injury. Our future work will investigate how functional connectivity change in the brain correlates with behavioral outcome after rmTBI at different impact sites.Acknowledgements
This study was funded in part by Ministry of Science and Technology (MOST 107-2314-B-038-005 and MOST 106-2218-E-039-001-MY3), Taipei, Taiwan.References
1. Aungst S L, Kabadi S V, Thompson S M, et al., Repeated mild traumatic brain injury causes chronic neuroinflammation, changes in hippocampal synaptic plasticity, and associated cognitive deficits. J Cereb Blood Flow Metab, 2014. 34(7): 1223-32.
2. Baugh C M, Kiernan P T, Kroshus E, et al., Frequency of head-impact-related outcomes by position in NCAA division I collegiate football players. J Neurotrauma, 2015. 32(5): 314-26.
3. Crisco J J, Fiore R, Beckwith J G, et al., Frequency and location of head impact exposures in individual collegiate football players. J Athl Train, 2010. 45(6): 549-59.
4. Mez J, Daneshvar D H, Kiernan P T, et al., Clinicopathological Evaluation of Chronic Traumatic Encephalopathy in Players of American Football. JAMA, 2017. 318(4): 360-370.
5. Simon D W, McGeachy M J, Bayir H, et al., The far-reaching scope of neuroinflammation after traumatic brain injury. Nat Rev Neurol, 2017. 13(3): 171-191.
6. Kao Y C J L, C.F.; Chen, C.Y., Behavioral and Image Evidence for Mild Traumatic Brain Injury in Rats with the Skull Helmet ISMRM Preceeding, 2017.
7. Kao Y C J L, C.F.; Chen, C.Y., Evolving Functional Connectivity in Rats following Mild Traumatic Brain Injury. ISMRM Preceeding, 2017.
8. Kao Y C J L, C.F.; Chen, C.Y., Low-frequency Fluctuations of Resting-state fMRI BOLD Signal after Experimental Mild Traumatic Brain Injury. ISMRM Preceeding, 2018.
Figures