0073
Pilot tone-based prospective respiratory motion correction for 2D cine cardiac MRI1Physikalisch-Technische Bundesanstalt (PTB), Braunschweig and Berlin, Germany, 2Siemens Healthcare, Erlangen, Germany
Synopsis
Respiratory motion during data acquisition can introduce strong motion artefacts in 2D cine cardiac MR images. The commonly used breathhold method minimizes these artefacts, but also limits achievable image resolution and requires patient cooperation. Here we present a prospective motion correction technique using RF pilot tone signals with high temporal resolution. A calibration scan was carried out to convert signal intensity changes of the pilot tone to displacements of the heart due to breathing. The proposed approach was evaluated in four healthy volunteers and allowed for free-breathing 2D cine MR with high image quality.
Introduction
Respiratory motion during data acquisition can introduce strong motion artefacts in 2D segmented cine MRI, where data is acquired over multiple cardiac cycles.
The commonly used breathhold method minimizes these artefacts, but also limits achievable image resolution and requires patient cooperation.1-2 Retrospective respiratory motion correction for cine MRI has been proposed previously.3 Nevertheless, this is challenging due to through-plane motion, which cannot be corrected retrospectively but requires prospective slice tracking. Commonly, slice tracking (i.e. adjusting the RF excitation pulse to compensate for heart movement due to breathing) uses a MR-based navigator monitoring the breathing motion of the liver.4 This is not applicable to cine MRI, because the MR-navigator would disrupt the continuous cine data acquisition.
Here we present an approach for free-breathing cine MRI that uses an RF pilot tone5-7 (PT) as a motion-surrogate to perform prospective respiratory motion correction via slice tracking. A short pre-scan is used to calibrate the PT signal. The obtained motion model is then used in the following cine acquisition to adapt the slice position to the current breathing phase in real-time. Calibration and slice tracking were implemented directly on the scanner and the feasibility of the approach is demonstrated in four healthy volunteers.
Methods
An overview of the calibration and motion correction method is given in Figure 1.
The method was implemented directly on a 3T scanner (MAGNETOM Verio, Siemens Healthcare, Erlangen, Germany). The PT signal was created by a prototype set-up similar to previous applications for respiratory gating and cardiac triggering.5-7 The signal was generated by a commercial RF-synthesizer (Hewlett Packard) connected to an additional inhouse-built non-resonant coil fixed to the bore of the scanner. The PT frequency was set such that the signal was recorded in the two-fold oversampled readout signal of the MR data. The PT signal intensity varied during respiration, thus providing a continuous, quantitative motion surrogate for each phase encoding point (i.e. with temporal resolution of TR). The PT signal was median filtered to ensure greater temporal stability.
In a first step, a calibration scan was performed over multiple respiratory cycles (approx. 1min). It consists of ECG-triggered, dynamic measurements using a b-SSFP sequence. For each cardiac cycle one coronal 2D-image was acquired to capture the respiratory translational motion of the heart (TE=1.5ms, TR=3.2ms, flip angle=30°, FOV=300x300mm2 and voxel size=1.56x1.56x5mm3). A normalized cross-correlation function was used to determine the respiratory displacement of the heart along foot-head direction. The PT signal was then calibrated to this displacement using a linear model. During the following 2D cine scans the foot-head translation of the heart due to breathing was estimated from the model and the location of the excited slice was adapted for each phase encoding step.
To evaluate the performance of the proposed approach, a dynamic MR acquisition in transverse orientation with the same scan parameters as the calibration scan was carried out during free-breathing, with and without PT slice tracking. In addition, 2D cine MR data was acquired during free-breathing, again with and without PT slice tracking. For reference purposes the 2D cine scan was also obtained during a single breathhold.
The method was applied to 4 volunteers (2 female, age 45 ± 19 years) after informed consent was obtained.
Results and Discussion
The pilot tone signal and registered heart position are very well synchronized and show good linear correlation with correlation coefficients R2 between 0.85 and 0.96 over all volunteers (Figure 2).
Figure 3 shows a comparison of dynamic 2D measurements without motion correction and with the slice tracking method. The pilot tone signal indicated a heart position change up to 9 mm in foot-head direction. This through-plane motion can be clearly seen in the uncorrected images. Free-breathing cine MRI without slice tracking shows strong breathing artefacts which are strongly reduced using the proposed technique (Fig. 4). Residual artefacts are due to the movement of the heart along anterior-posterior or left-right, which have so far not been corrected here.
Conclusion
Here we presented a prospective respiratory motion correction approach to compensate for through-plane motion in 2D cine MRI. A pilot tone signal was correlated to respiratory heart motion and the linear correlation parameters were then used to derive prospective motion correction information (i.e. slice tracking shift). We demonstrated that the pilot tone signal could be used as a quantitative motion surrogate and translational slice tracking was successfully applied during measurements resulting in improved image quality of transversal 2D cardiac cine scans.Acknowledgements
No acknowledgement found.References
[1] Scott A D, et al., 2009. Motion in Cardiovascular MR Imaging. Radiology: Volume 250: Number 2 – February 2009.
[2] McClelland J R, et al., 2013. Respiratory motion models: A review. Medical Image Analysis 17, p. 19-42.
[3] Hansen M S, et al., 2012. Retrospective reconstruction of high temporal resolution cine images from real-time MRI using iterative motion correction. Magnetic Resonance in Medicine, 68(3), pp.741–750.
[4] Wang Y, et al., 1995. Respiratory motion of the heart: kinematics and the implications for the spatial resolution in coronary imaging. Magnetic Resonance Imaging, 33(5), pp.713–719.
[5] Speier S, et al., 2015. PT-Nav: A Novel Respiratory Navigation Method for Continuous Acquisition Based on Modulation of a Pilot Tone in the MR-Receiver. ESMRMB 129:97-98, 2015. Doi: 10.1007/s10334-015-0487-2.
[6] Bacher M, et al., 2018. Model-Based Lag Free Processing of Pilot Tone Navigator Data Enables Prospective Cardiac Triggering. Proc. ISMRM 2018, #2960.
[7] Schroeder L, et al., 2016. Two-Dimensional Respiratory-Motion Characterization for Continuous MR Measurements Using Pilot Tone Navigation. In Proc. Intl. Soc. Mag. Reson. Med. 24:310.
Figures
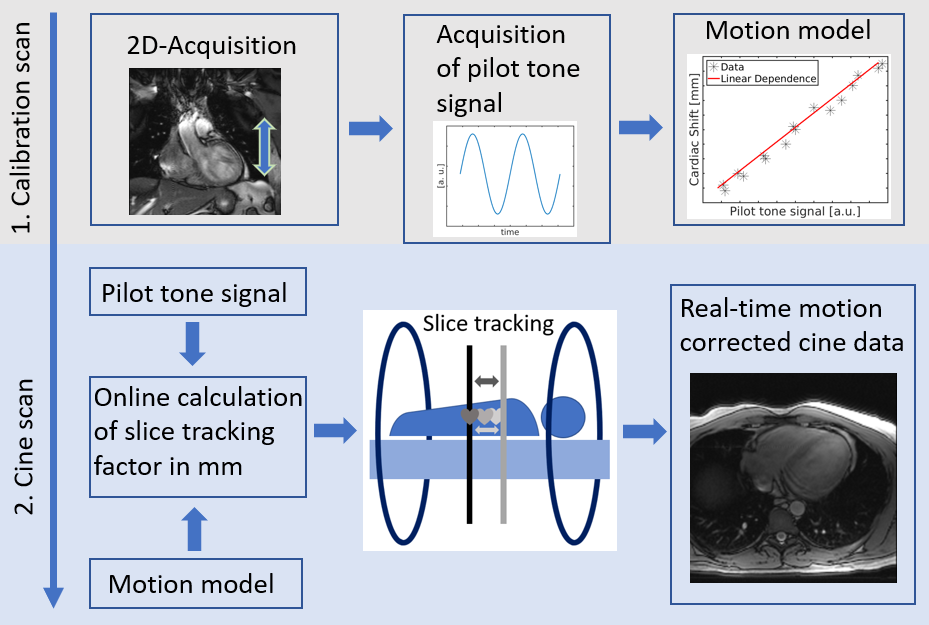
Figure 1: Overview of the proposed two-step method. First, simultaneous acquisition of MR data and pilot tone data is carried out for about 1 min to calibrate the pilot tone signal to the respiratory motion of the heart and derive a motion model. The data of subsequent 2D cine scans can then be motion corrected prospectively during acquisition using the motion model and the pilot tone data and adapting the location of the excited slice.
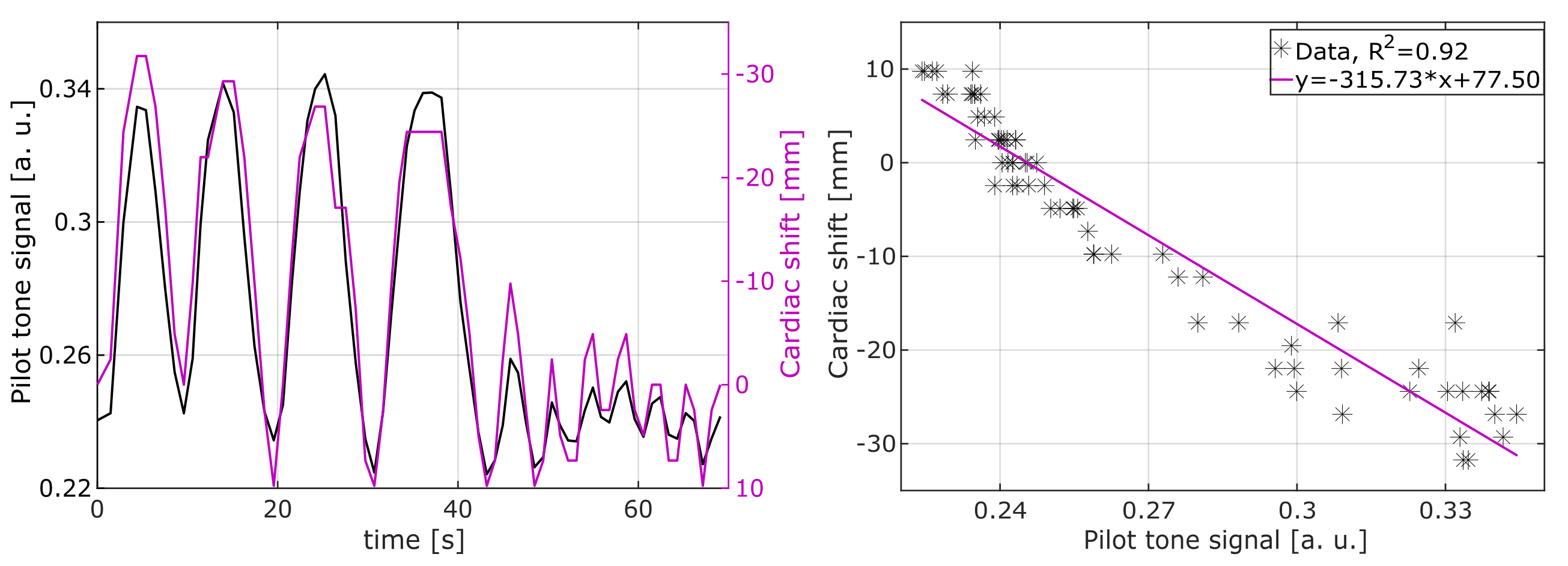
Figure 2: Left: The median pilot tone signal and the registered heart motion (cardiac shift) from the 2D calibration scan show very good temporal correlation. The volunteer was asked to perform deep breathing followed by normal breathing. Right: Pilot tone and cardiac shift correlate well using a linear model with a correlation coefficient of 0.92.
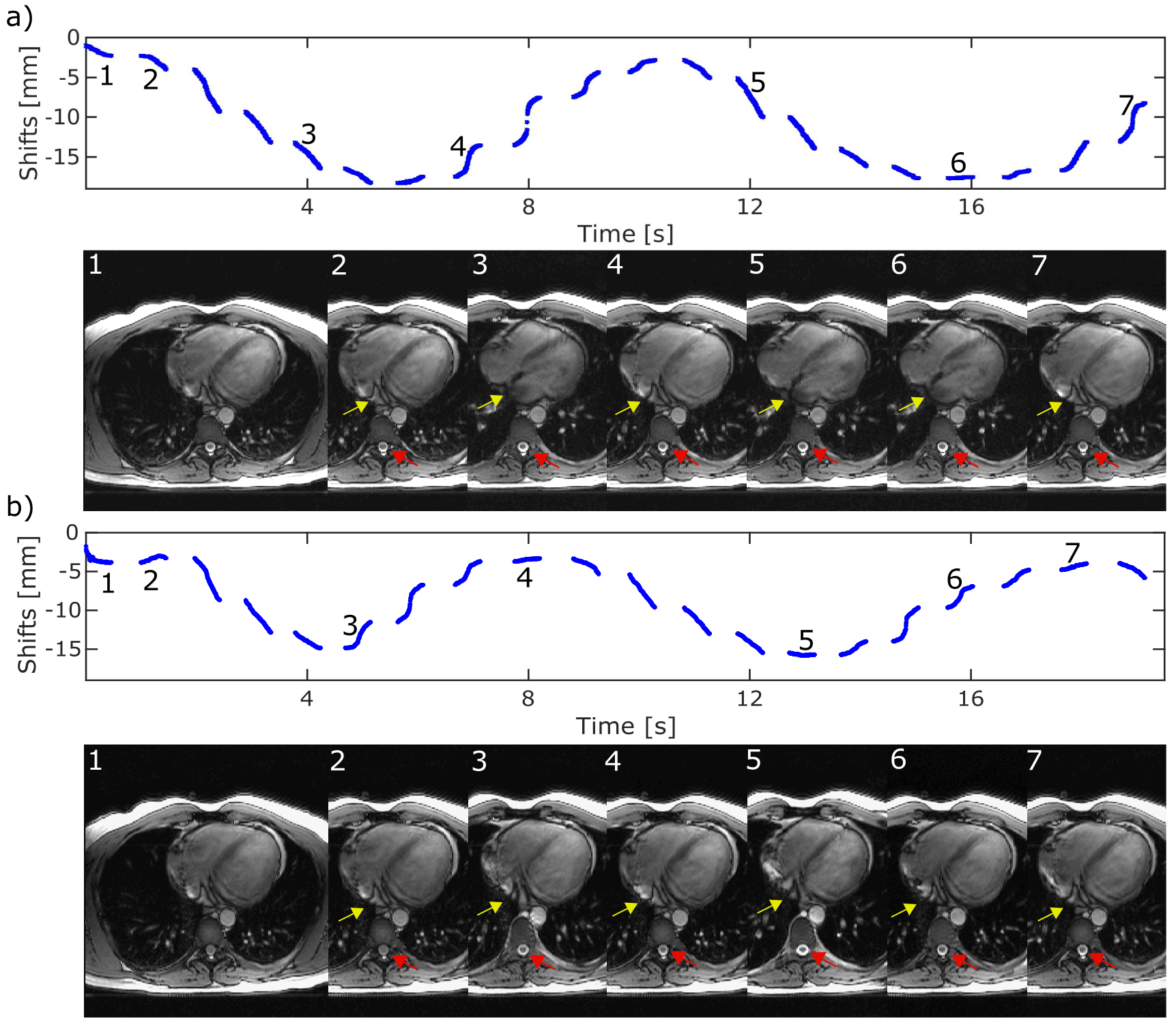
Figure 3: Two dimensional dynamic scans with 20 repetitions a) without slice tracking and b) with slice tracking. The heart motion (shift) was derived from the PT signal for both scans. MR images from seven different respiratory motion states are depicted. Position curves are not smooth because the PT signal was median filtered. The through plane motion of the heart was minimized with the slice tracking method. a) Respiratory heart motion through image plane can be clearly seen (yellow arrow). The applied slice shift in b) can be seen clearly as a change of the anatomy around the vertebra (red arrow).
Figure 4: 2D cine scans for two volunteers. Free breathing acquisitions without correction reveal strong motion artefacts (a) and c)). Images obtained during free breathing with slice tracking show a reduction of the motion artefacts (b) and d)). Residual artefacts are due to motion along left-right and/or anterior-posterior which so far has not been corrected for. e) shows the gold standard breathhold method. Residual artefacts of the pilot tone can be seen in the center of the FOV.