0070
Free-breathing placental and fetal MR angiography using continuous stable state acquisition (Sweep)1Biomedical Engineering,School of Biomedical Engineering & Imaging Sciences, Kings College London, London, United Kingdom, 2Department of Women and Children’s Health, School of Life Course Sciences, Kings College London, London, United Kingdom, 3Centre for the Developing brain, School of Biomedical Engineering & Imaging Sciences, Kings College London, London, United Kingdom
Synopsis
Major obstetric complications such as pre-eclampsia and intrauterine growth restriction can result from malformations in the circulation of the fetus and placenta. Robust, high resolution in-utero MR angiography has the potential to be a valuable tool in identification and monitoring of these disorders but is hampered by the presence of complex motion, ineffective breath holds and lack of safe contrast agents. Here we present a motion compensated method for visualising the vascular networks in the fetus and placenta using respiration resolved 2D inflow angiography with efficient and dense spatiotemporal sampling and retrospective correction.
Introduction
The developing fetal vascular system including its complex integration with maternal circulation through the placenta is fundamental to fetal wellbeing. The origin of major obstetric complications such as pre-eclampsia and fetal growth restriction can be traced to placental vascular impairment.1 In-utero magnetic resonance angiography (MRA) of fetus and placenta is a complex problem. Non-periodic motion originating independently from both maternal and fetal sources prevent the use of conventional 3D MRA methods. Imaging during pregnancy also prohibits the use of vascular contrast agents and reduces patient compliance to breath hold acquisitions.
RF-spoiled gradient echo acquisitions (SPGR) with high flip angles can utilise steady state saturation and inflow enhancement to produce effective non-contrast angiography. In the case of fetal imaging these sequences must be acquired using 2D snapshots to minimise artefacts from unpredictable fetal motion.2
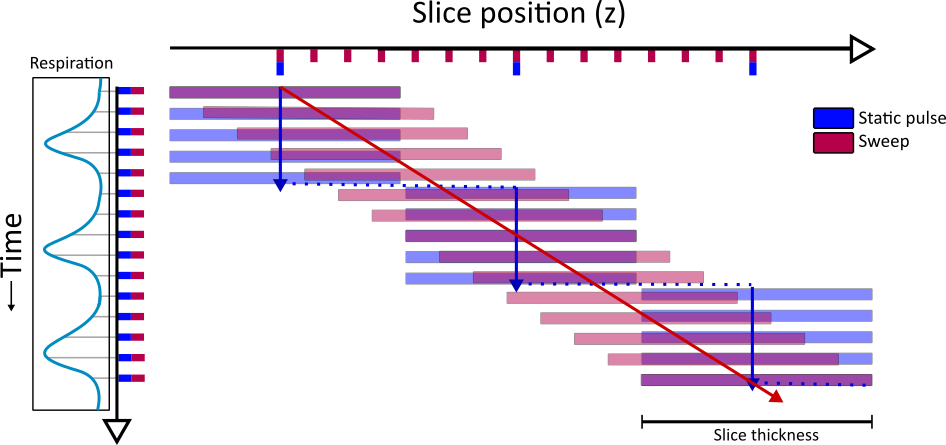
In this work we use a linear offset in RF pulse frequency every TR such that each pulse excites a pulse profile slightly displaced in the slice direction (z).3 This RF ‘sweep’ approach has a number of advantages when applied to 2D MRA. 1) Although the slice profile never enters a true steady state, since each pulse contains unexcited tissue, a stable signal state is achieved in the background tissue, this signal then remains consistently suppressed without the need for dummy cycles. 2) All sampling is temporally and spatially close, limiting the potential for major fetal motion to corrupt an acquisition, and ensures information at a local scale is geometrically consistent. 3) Resolving respiration in free-breathing MRI typically requires a series of samples/dynamics across the respiratory cycle for each spatial location.4 In the sweep approach, each of these samples are spatially offset, meaning that z is sampled more densely than in conventional static pulse methods (Figure 1).
Methods
Imaging was performed on a Philips 3T Achieva system equipped with a 32-channel cardiac RF coil. Informed consent was obtained from 8 pregnant volunteers as part of the Placenta Imaging Project (PIP) (Gestational age (GA): 21-32w). Scanning was performed in the supine position with routine blood pressure and pulse oximetry monitoring. No sedation, gating or exogenous contrast methods were used.
A flow-compensated multislice 2D SPGR acquisition was performed with RF spoiling to produce time-of-flight contrast. Matched scans were performed using both the conventional static pulse and sweep approaches. Relevant acquisition parameters were FOV=260x320x220mm; Resolution=1.2x1.2mm; slice thickness=3.5mm; TR/TE=10/5.4ms; flip=55⁰; SENSE=2; sweep shift/pulse=6.4µm; time/slice=580ms; Total acquisition time=5:33m.
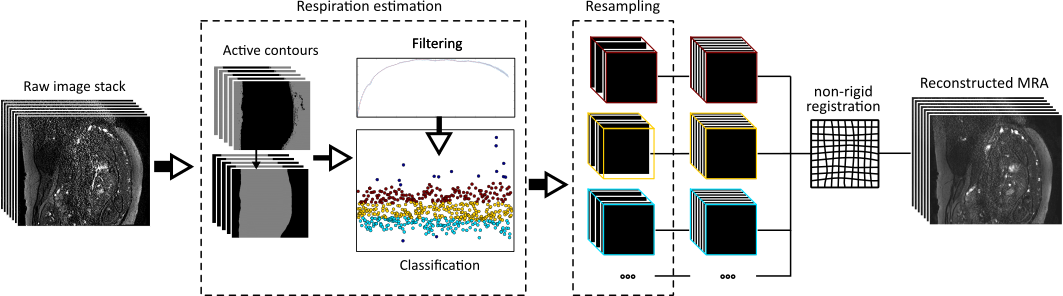
The proposed motion correction pipeline applied to these images is depicted Figure 2, all analysis was performed in Matlab and MIRTK.5 In brief, individual slices were binned into respiration states based on the local variation in body area following an active-contour based automatic segmentation.6 Respiration resolved volumes were then constructed from these binned slices. These volumes were then co-registered into a single isotropic volume using a non-rigid normalised mutual information registration.
Results
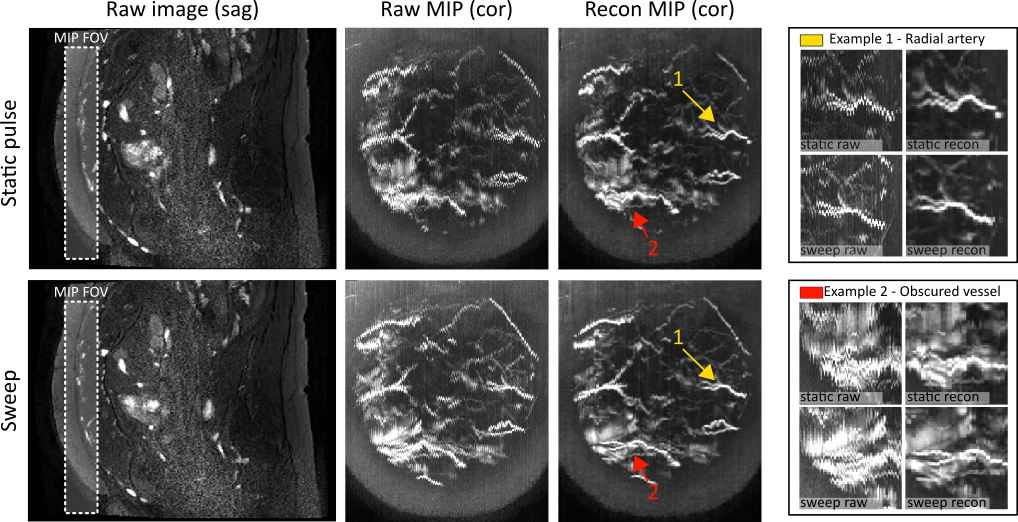
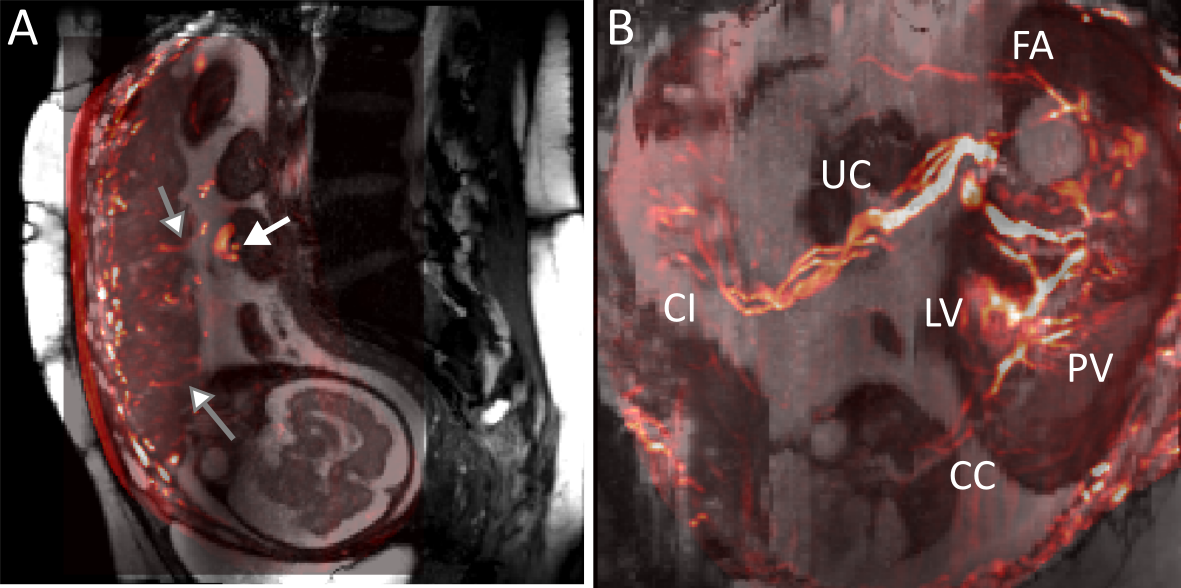
A comparison of conventional static pulses and the proposed sweep method is shown in a healthy subject (GA: 31w) (Figure 3). Although temporal sampling is identical, the sparseness of the spatial sampling with the static pulse method limits the effectiveness of the motion correction compared to the sweep acquisition. Figure 4 shows a healthy control (GA: 28w). In this case an anatomical overlay provides local image context. The resulting angiogram shows several major vascular features in the placental parenchyma and fetus.
Discussion
The described methods produce free breathing and contrast free abdominal MRA in the challenging pregnant subject. The resulting images show clearly defined vessels without the severe respiration artefacts present in the raw data.
The proposed method does not correct for large unpredictable fetal displacement, instead the dense spatiotemporal sampling means that all image information is consistent at a local scale. In-utero angiography has previously been considered at late gestations (GA>=36w) to limit potential for fetal motion.2 The proposed method builds on this by introducing motion correction and increasing the spatial sampling density, creating a more robust acquisition that is effective at earlier gestations (GA>=21w), an important factor in intervention and treatment planning. Limitations of the current methods are that the acquired data is sensitive only to flow in the through plane direction, which is a limitation of inflow MRA generally. A potential solution to this is to incorporate orthogonal acquisitions from the transverse and coronal planes with a slice-to-volume registration technique combining the resolved volumes.7
Conclusion
The described methods produce free breathing and contrast free abdominal MRA in the pregnant subject. These images may be valuable for detecting vascular abnormalities in the fetus or placenta before the onset of obstetric complications. Although these techniques have been developed for the fetal angiography case they are widely applicable to abdominal imaging in general.Acknowledgements
This work was supported by the NIH Human Placenta Project grant 1U01HD087202-01 (Placenta Imaging Project (PIP)), the Wellcome Trust (Sir Henry Wellcome Fellowship, 201374/Z/16/Z), and the EPSRC (grants N018702 and M020533) and by the National Institute for Health Research (NIHR) Biomedical Research Centre based at Guy’s and St Thomas’ NHS Foundation Trust and King’s College London. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health.References
1. Campbell, S. Placental vasculature as visualized by 3D power Doppler angiography and 3D color Doppler imaging. Ultrasound Obstet. Gynecol. 30, 917–920 (2007).
2. Neelavalli, J. et al. Magnetic resonance angiography of fetal vasculature at 3.0 T. Eur. Radiol. 26, 4570–4576 (2016).
3. Jackson, L. H. et al. Respiration resolved imaging using continuous steady state multiband excitation with linear frequency sweeps. Proc. ISMRM18 Paris (2018).
4. Cai, J., Chang, Z., Wang, Z., Paul Segars, W. & Yin, F. F. Four-dimensional magnetic resonance imaging (4D-MRI) using image-based respiratory surrogate: A feasibility study. Med. Phys. 38, 6384–6394 (2011).
5. Schnabel, J. A. et al. A generic framework for non-rigid registration based on non-uniform multi-level free-form deformations. in Lecture Notes in Computer Science (including subseries Lecture Notes in Artificial Intelligence and Lecture Notes in Bioinformatics) (2001). doi:10.1007/3-540-45468-3_69
6. Chan, T. F. & Vese, L. A. Active contours without edges. IEEE Trans. Image Process. 10, 266–277 (2001).
7. Kuklisova-Murgasova, M., Quaghebeur, G., Rutherford, M. A., Hajnal, J. V. & Schnabel, J. A. Reconstruction of fetal brain MRI with intensity matching and complete outlier removal. Med. Image Anal. 16, 1550–1564 (2012).
Figures