0042
Brain Microstructural Changes Support Cognitive Deficits in Normal Children Born to HIV-infected Mothers1Division of Translational Medicine, Sidra Medicine, Doha, Qatar, 2Department of Radiology and Imaging, Fortis Memorial Research Institute, Gurgaon, India, 3Department of Neurology, King George Medical University, Lucknow, India, 4Department of Microbiology, King George Medical University, Lucknow, India, 5Department of Psychiatry, Sidra Medicine, Doha, Qatar, 6Laboratory Animal Research Center, Qatar University, Doha, Qatar
Synopsis
In the current study, we evaluated the brain integrity [by mapping the fractional anisotropy (FA) and mean diffusivity (MD)] and neurocognitive performance (NP) in normal children (NCI) born to HIV-infected mother compared to normal children (NCH) born to healthy mother and HIV-infected children (HI). Reduced FA in multiple brain sites of HI and NCI children suggests loss of tissue integrity while altered MD indicates presence of cerebral edema. Presence of tissue changes and abnormal cognition in absence of HIV-infection in NCI children advice that ART may have detrimental effects on brain.
Introduction:
Perinatal HIV infection is a growing problem worldwide. The early inception of antiretrovirals therapy (ART) helps to improve clinical, immunological, and developmental outcomes[1-3]. Because of the reported neurotoxic effect of ART few studies evaluated the brain changes and neurocognitive performance in normal children (NCI) born to HIV-infected mother underwent ART[4,5]. They observed significant brain changes and neurocognitive deficits in NCI compared to the children born (NCH) to healthy mother. So far, there is no comprehensive study investigating the white matter and gray matter changes in association with the neurocognitive performance (NP) in NCI subjects. In the current study, we assessed the brain’s microstructural tissue integrity using diffusion-tensor-imaging (DTI), and NP in NCI children compared to NCH and HIV-infected children (HI).Materials and Method:
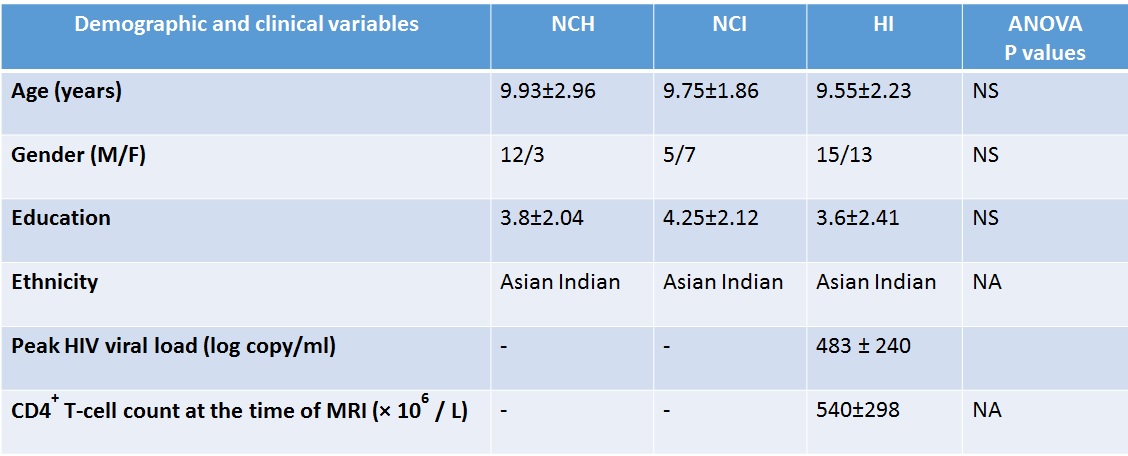
Institutional regulatory board approved the current study protocol. 59 HI, 15 NCH, and 12 NCI children were recruited. Diagnosis of HIV was performed under national HIV testing protocol. With informed consent, each child underwent NP test using Revisie Amsterdamse Kinder Intelligentie Test battery, and brain MRI on a 3-T GE scanner using an 8 channel head coil. Conventional (T1-, T2- and FLAIR), high-resolution T1-weighted and DTI images were acquired from each subject. For DTI, dual spin-echo single-shot echo-planar sequence with 30 uniformly distributed directions with ramp sampling was used: TR=17 sec, TE=88.7 ms, slice thickness=3 mm, intersection gap=0, FOV=240×240 mm, image matrix=256×256, NEX=1, diffusion-weighting b-factor=1000s/mm2, slice number=46. Based on the conventional MRI findings, 15 HI children showed hyperintensity on T2-weighted and FLAIR images were excluded from the study. Because of the motion artifact another 16 HI children were excluded from the analysis. Final analysis was performed on 28 HI, 15 NCH and 12 NCI children.
DTI Processing: DTIStudio (v.3.0.3) was used for quantification of DTI metrics as described in detail elsewhere[6]. Motion correction was performed using Automated Image and Registration package implemented in DTIStudio. Diffusion tensor matrices were calculated using DWIs collected from gradient and b0 images. From the diffusion tensor images, fractional anisotropy (FA) and mean diffusivity (MD) maps were constructed.
Normalization and Smoothing of FA and MD Maps: Statistical parametric mapping package (SPM12) was used for the voxel based analysis (VBA). Briefly, non-diffusion weighted images of individual subject were normalized to the Montreal Neurological Institute (MNI) space, using a prior defined distribution of tissue probability maps, and the resulting normalization parameters were applied to the corresponding FA and MD maps and these maps were smoothed using a Gaussian filter full-width-at-half-maximum of 10mm and used for VBA.
Statistical Analysis: IBM Statistical Package for the Social Sciences (v.18) software was used to examine the demographic, clinical, and NP scores using ANOVA and Chi-square. Analysis of covariance (ANCOVA; covariates: age and gender) was performed to see the voxel wise difference in FA and MD maps among the groups, (with uncorrected threshold, p<0.001; minimum extended cluster size, 150 voxels).
Results:
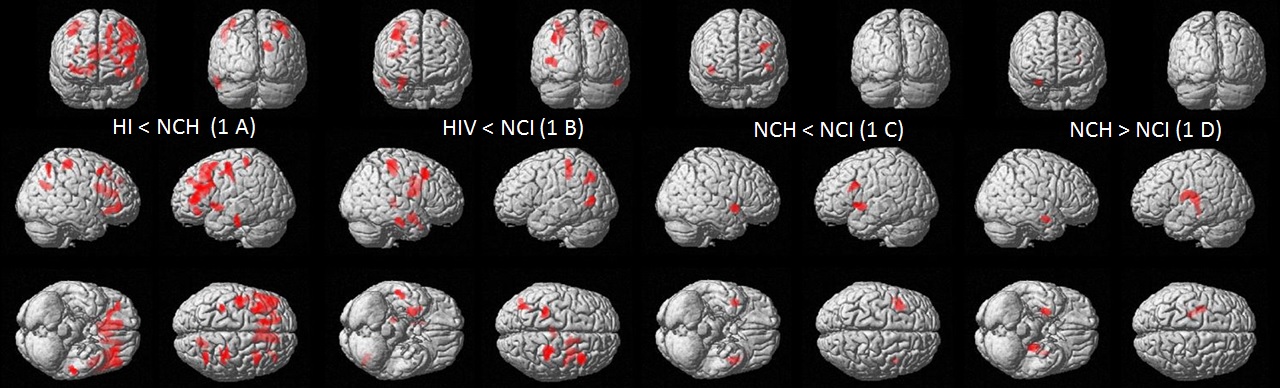
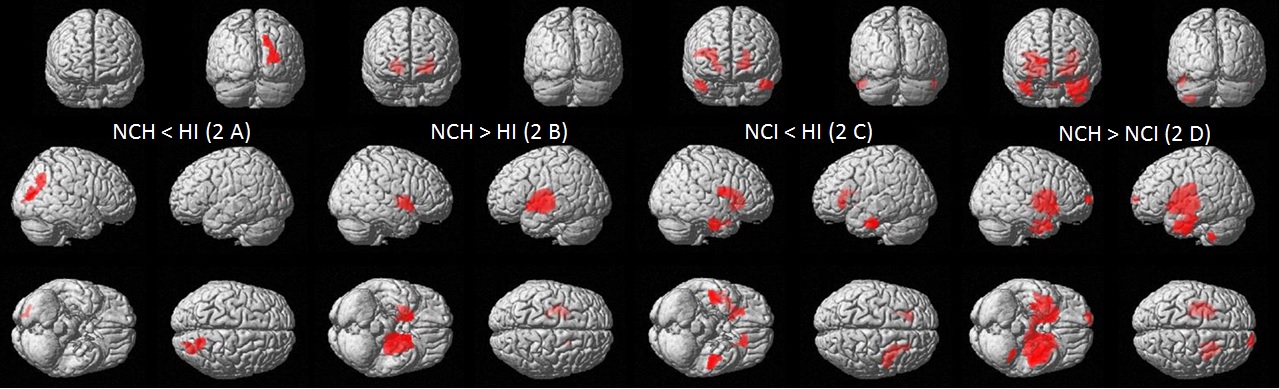
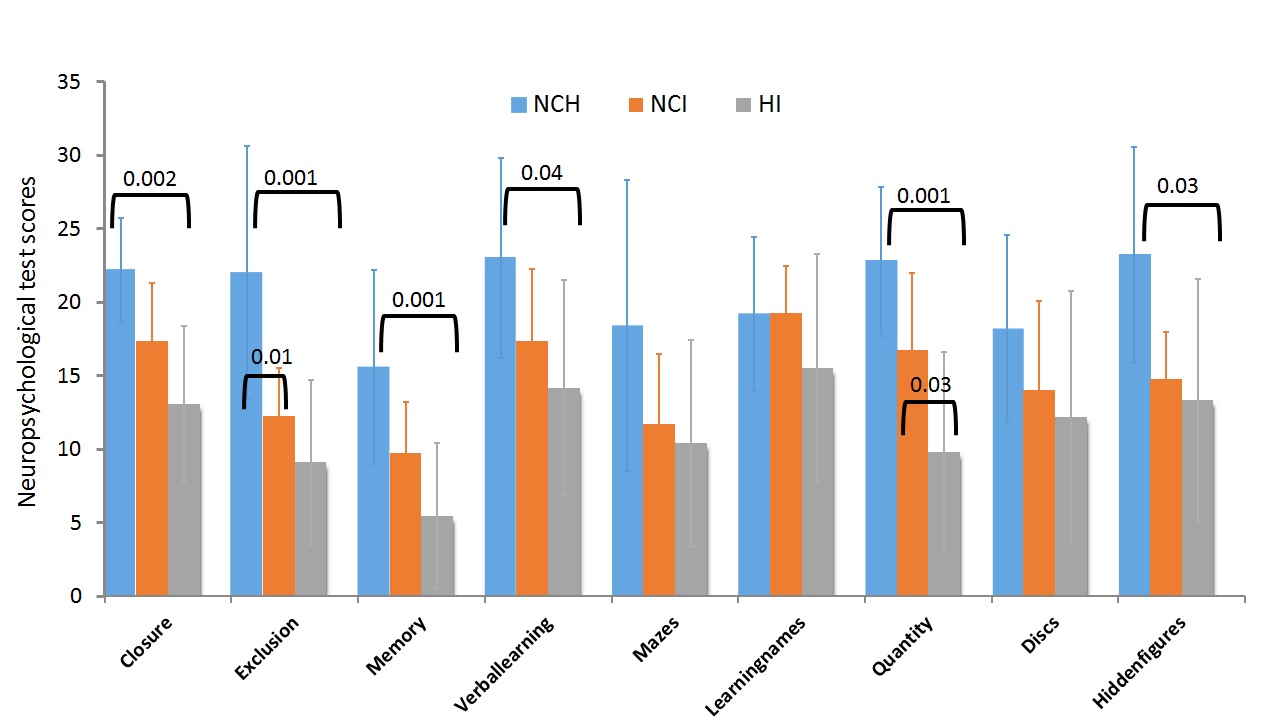
Demographic, and clinical parameters of subjects are summarized in table 1. HI children showed significantly altered NP test score in 5 domains, while NCI children showed abnormal NP test score in 2 domains as compared to NCH (Figure 3). Significantly reduced FA was observed in frontal, temporal, occipital, and parietal gray and white matter, and in limbic region of HI children compared to NCH children (Figure 1A). HI children showed significantly decreased FA in frontal, temporal, and parietal gray and white matter, corpus callosum, limbic region, right thalamus and right insular cortex compared to NCI children (Figure 1B). NCI children showed significantly altered FA in frontal white matter, bilateral insular cortices, extra-nuclear and right limbic region (Figure 1C & D) compared to NCH children. MD values were significantly reduced in the left extra-nuclear and right lentiform nucleus, and significantly increased in the right parietal region of HI children compared to NCH children (Figure 2A). Significantly higher MD values were observed in frontal and temporal regions, and right extra-nuclear of HI children compared to NCI children (Figure 2B). MD values were significantly increased in bilateral lentiform nucleus, left pons, and left posterior lobe of NCH children compared to NCI children (Figure 2D).Discussion and Conclusion:
Reduced FA in multiple brain sites of HI and NCI children suggests loss of tissue integrity while altered MD indicates presence of cerebral edema. Presence of abnormal tissue integrity and cerebral edema might be responsible for deficit in the neurocognitive functions in HI and NCI children. Presence of tissue changes and abnormal NP scores in absence of HIV infection in NCI children emphasize that ART may have detrimental effects on brain.Acknowledgements
Sidra Medicine, Doha, Qatar, has provided the workstation for image processing.References
1. Laughton B, Cornell M, Grove D, Kidd M, Springer PE, et al. (2012) Early antiretroviral therapy improves neurodevelopmental outcomes in infants. AIDS 26: 1685-1690. 2. Zheng J, Zhao D (2014) Clinical, immunological, and virological outcomes of pediatric antiretroviral therapy in central China. BMC Res Notes 7: 419. 3. Laughton B, Cornell M, Kidd M, Springer PE, Dobbels EFM, et al. (2018) Five year neurodevelopment outcomes of perinatally HIV-infected children on early limited or deferred continuous antiretroviral therapy. J Int AIDS Soc 21: e25106. 4. Nwosu EC, Robertson FC, Holmes MJ, Cotton MF, Dobbels E, et al. (2018) Altered brain morphometry in 7-year old HIV-infected children on early ART. Metab Brain Dis 33: 523-535. 5. Robertson FC, Holmes MJ, Cotton MF, Dobbels E, Little F, et al. (2018) Perinatal HIV Infection or Exposure Is Associated With Low N-Acetylaspartate and Glutamate in Basal Ganglia at Age 9 but Not 7 Years. Front Hum Neurosci 12: 145. 6. Jiang H, van Zijl PC, Kim J, Pearlson GD, Mori S (2006) DtiStudio: resource program for diffusion tensor computation and fiber bundle tracking. Comput Methods Programs Biomed 81: 106-116.Figures