0030
Using convolutional neural networks to predict infarct development in acute ischemic stroke patients: does reperfusion status matter?Yuan Xie1, Yannan Yu1, Thoralf Thamm1, Charles Huang1, Enhao Gong1, Soren Christensen1, Maarten Lansberg1, and Greg Zaharchuk1
1Stanford University, Stanford, CA, United States
Synopsis
Convolutional Neural Network has shown promising results in stroke treatment outcome predictions. Our study explores the hypothesis of whether training a CNN model with patients who have similar treatment outcomes can improve the model prediction of day 5 stroke lesion.
Introduction
For acute ischemic stroke (AIS) patients, predicting final infarction is a key element for triage. Using input data from baseline multimodal MRI, deep learning models have been found useful in final infarct prediction (Nelson et al.). However, the patient’s reperfusion treatment outcome can greatly influence the actual prognosis. In this study we investigated whether knowledge of the patient’s reperfusion status improves deep-learning-based prediction performance.Methods
AIS patients were reviewed and selected from the prospective, multi-center Imaging Collaterals in Acute Stroke (iCAS) and DEFUSE2 studies. We included patients who underwent baseline MRI including perfusion-weighted imaging with dynamic susceptibility contrast (DSC), diffusion-weighted imaging (DWI), and gradient echo (GRE) imaging; and follow up imaging with T2-FLAIR performed 3-5 days after stroke onset. The ground truth was defined as the stroke lesions on follow-up T2-FLAIR, which were manually delineated by readers blinded to clinical information. Perfusion maps (Tmax, cerebral blood flow, cerebral blood volume, and mean transient time) were reconstructed by RAPID software (IschemaView, Redwood City, CA). All images were co-registered to Montreal Neurological Institute template space with SPM software. Three U-Net models were trained with the above-mentioned 7 different contrasts as inputs (Figure 1). The first model was trained on 50 reperfused patients, the second on 50 non-reperfused patients and the third on 50 patients randomly selected from previous two training sets, with 25 reperfused and 25 non-reperfused patients. Reperfusion was determined based on follow-up DSA images by neurointerventional radiologists based on a TICI score of >= 2b. The models were trained based on a mixed loss function of cross-entropy and SSIM. The three models were evaluated on a test set with 26 patients, 13 reperfused and 13 non-reperfused patients. The predictions and the results are reported as area under the receiver operator curve (AUC), Dice score, and predicted stroke volumes.Results
The study included a total of 126 patients (63 males, age 65±16, baseline NIHSS 15±6). 7 patients received IV tPA only, 57 with IV tPA plus thrombectomy, 33 with thrombectomy only, and 4 without reperfusion therapy. Overall, the model trained on non-reperfusers showed a significantly higher Dice score (0.47±0.047, pval = 0.045) and AUC (0.94±0.0021, pval = 0.00069) than the model trained on reperfused patients (Table 1). Comparing between the reperfused and non-reperfused test sets, the reperfused model had a significantly higher AUC when tested on reperfused patients (0.93±0.0016, pval = 0.013), in comparison to testing on non-reperfused patients (0.89±0.0029). When predicting reperfused stroke lesion volumes, (Figure 2) non-reperfused model shows highest correlation with ground truth volume (R = 0.669). The largest volume error is 271.4 cm3 predicted by the reperfused model on non-reperfused test set.Discussion
Grouping patients into reperfused vs. non-reperfused subgroups with targeted models trained on similar cohorts improves prediction AUC for reperfused patients. In addition, an overall higher Dice score is observed for the non-reperfused model predictions. This may be due to more uniformed lesion outcomes in non-reperfused cases compare to outcomes in reperfused cases, where reperfusion of the affected territory can range from 50% (TICI score of 2b) to 100% (TICI score of 3).Conclusion
Deep learning models trained using patients with the same reperfusion results does not uniformly improve the prediction outcome of stroke lesions on similar patients in the test set, a surprising finding that requires further investigation.Acknowledgements
No acknowledgement found.References
1. Nielsen A, Hansen MB, Tietze A, Mouridsen K. Prediction of Tissue Outcome and Assessment of Treatment Effect in Acute Ischemic Stroke Using Deep Learning. Stroke 2018;49:1394-1401.Figures
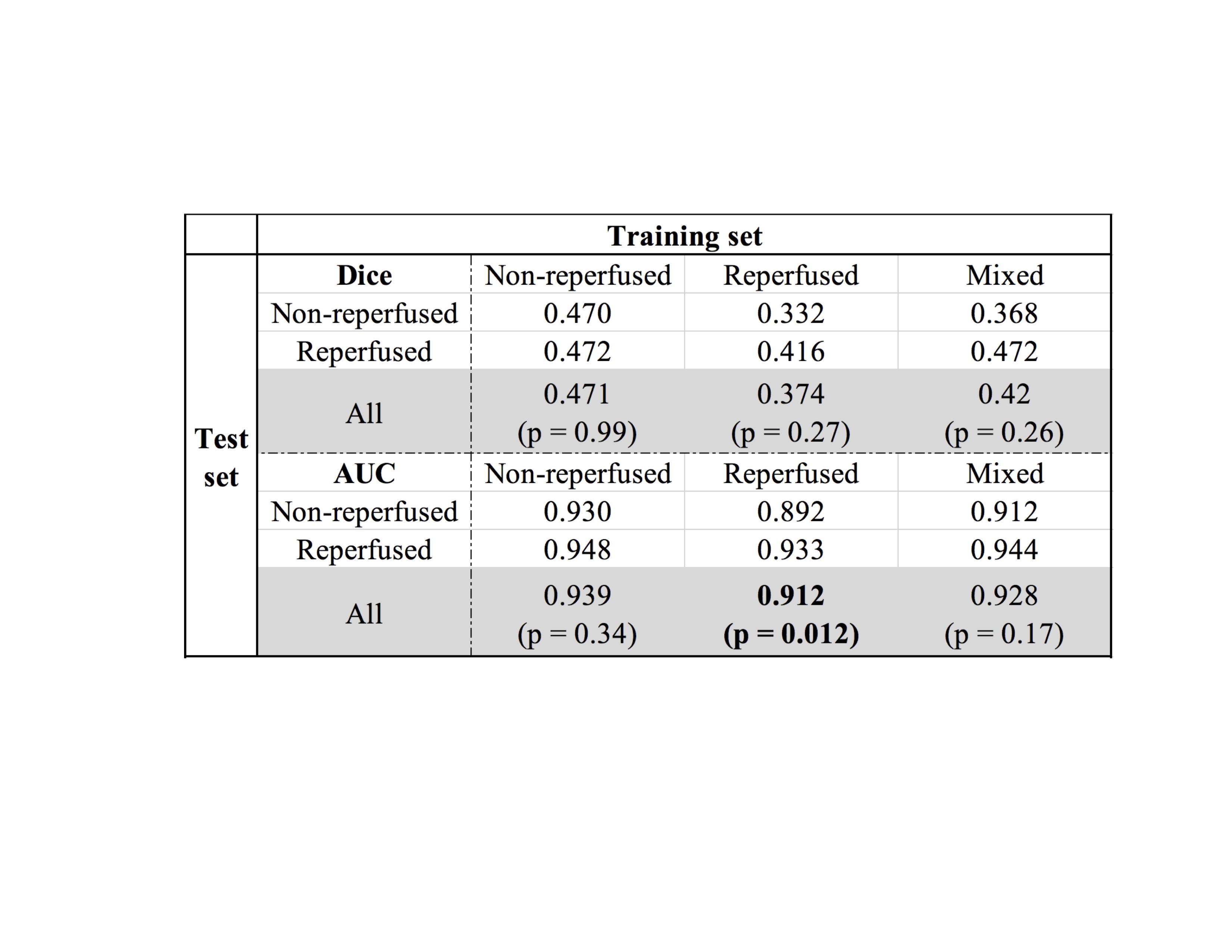
Table1.
This table shows Dice and AUC for the models trained on three training sets (n
= 50) and tested on reperfused,
non-reperfused
test sets (n=13) and both test sets combined (n = 26). Only AUC from the reperfused
model showed a significant increase when testing on reperfused
test set.
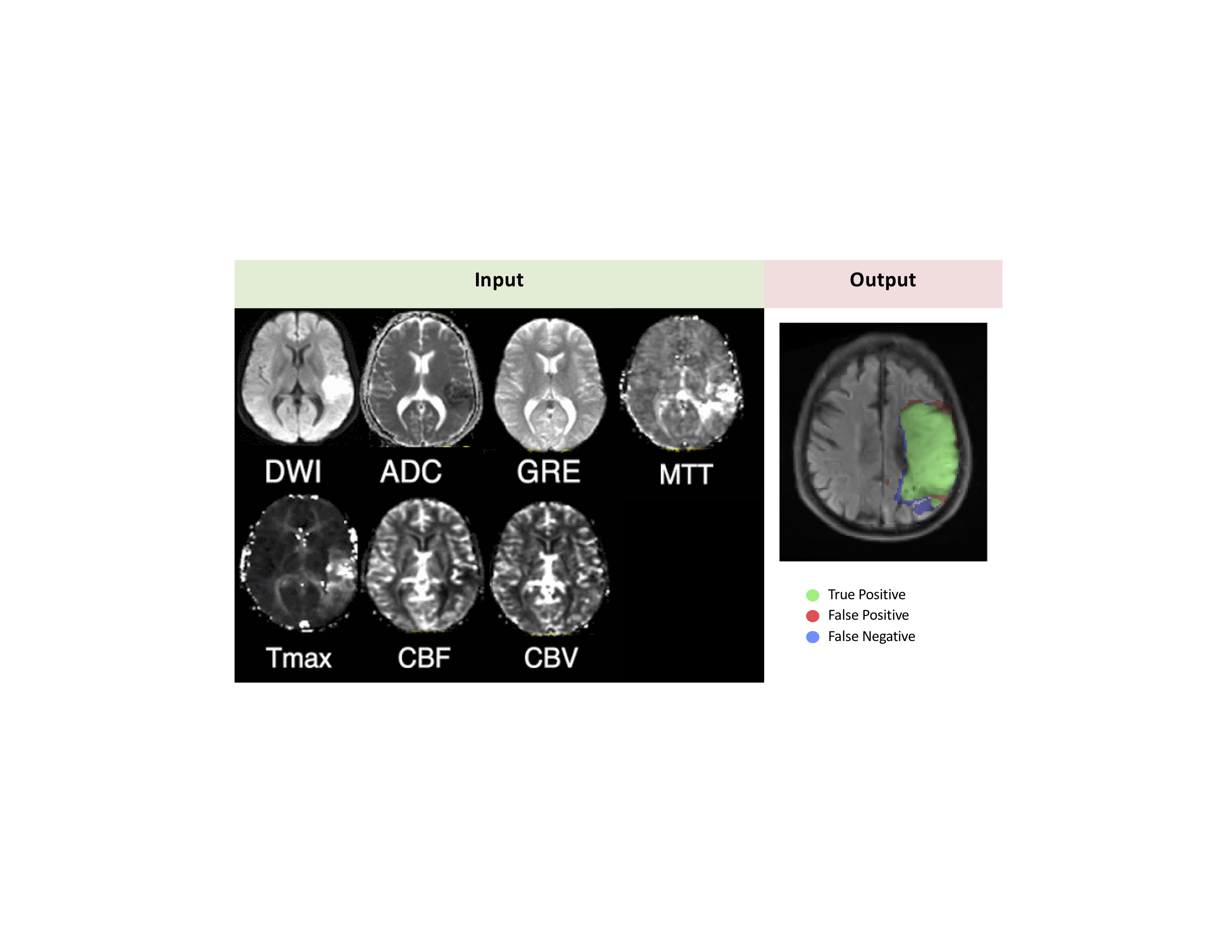
Figure1. The model takes in 7 contrasts as input, and predicts a lesion segmentation that is then compared with ground truth segmentation drawn by trained experts.
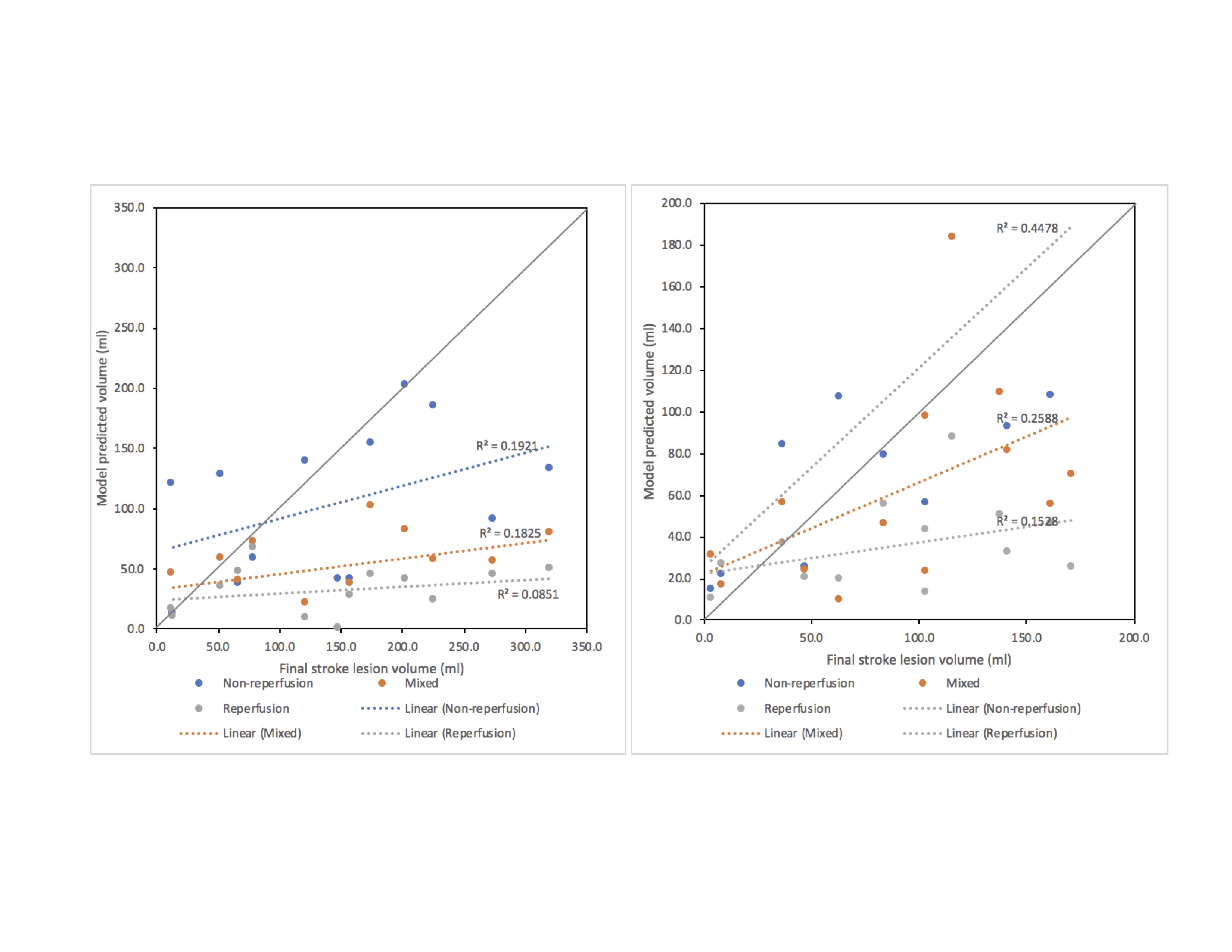
Figure 2. Correlation plot between model predicted lesion volume and ground truth stroke lesion volume. Figure A shows the correlation outcome in non-reperfused test set. Figure B shows outcome in reperfused test set. Predicted volumes from non-reperfused model have the highest correlation with both test sets in comparison to other models.