0013
Combined ventilation and perfusion imaging using dynamic susceptibility contrast 19F-MRI of inhaled perfluoropropane1Newcastle Magnetic Resonance Centre, Institute of Cellular Medicine, Newcastle University, Newcastle upon Tyne, United Kingdom, 2Institute of Cellular Medicine, Newcastle University, Newcastle upon Tyne, United Kingdom
Synopsis
19F-MRI of inhaled perfluoropropane (PFP) can be used to assess pulmonary ventilation. PFP has a short in vivo T2* (~2ms) arising from magnetic field inhomogeneity in the lung, reflecting the different magnetic susceptibilities of adjacent alveolar walls and gas components. Intravenous injection of a paramagnetic contrast agent to the pulmonary circulation can transiently reduce these magnetic susceptibility gradients, raising the T2* of inhaled PFP in regions directly adjacent to well-perfused lung. We present the first in man demonstration of combined pulmonary ventilation and perfusion assessment using 19F-MRI of inhaled PFP with concurrent administration of a gadolinium-based contrast agent.
Introduction
19F-MRI of inhaled perfluoropropane mixed with 21% oxygen (PFP/O2) is an emerging approach to ventilation imaging in humans. However, the technique remains challenging owing to a short in vivo T2* (~2ms, reduced from T2*=12ms in a magnetically homogeneous environment1) arising from magnetic susceptibility differences at the gas-tissue interfaces. Previous preclinical studies have reported the ability to alter the magnetic susceptibility of lung tissue towards that of the airspaces using intravenously-administered paramagnetic contrast agents2,3. We hypothesised that intravenous administration of a gadolinium-based contrast agent (GBCA) would reduce the magnetic susceptibility differences between adjacent vascular and gas components, and that this change would produce a sufficient rise in perfluoropropane T2* to permit assessment of alveolar perfusion. Consequently, we tested whether dynamic susceptibility contrast (DSC) 19F-MRI of inhaled PFP has potential utility for performing combined lung ventilation/perfusion measurement. We measured the impact of GBCA administration on PFP T2* in lung-representative phantoms, and performed DSC-19F-MRI studies in healthy volunteers to test feasibility of this approach.Methods
The impact of Gadobutrol concentration on the T2* of neighbouring PFP gas was investigated in phantom test objects. Lung-representative phantoms were fabricated to reflect the microstructure, gas-tissue ratio and magnetic susceptibility gradients present in lung tissue. This was achieved with an aqueous foam, with a PFP gas component and an aqueous component made from a 1:6 (w/w) ratio of pasteurized egg white powder (Dr Oetker Ltd., UK) and water. The foam was produced by repeatedly passing the gas and aqueous components between a pair of syringes through an approximately 1mm diameter restriction. The magnetic susceptibility of the aqueous component was altered by the addition of Gadobutrol (Bayer Schering Pharma, UK). Phantoms were produced with an aqueous component containing Gadobutrol at five concentrations ranging from 0 to 60mM (three samples at each concentration). MR relaxation properties of the PFP in each sample were measured using a 25mm diameter solenoid RF coil interfaced to a Philips Achieva 3T scanner. The T2* of PFP was determined by fitting a decaying exponential to the amplitude of a 19F pulse-acquire free induction decay (TR=34ms, θ=90o, 10 averages) acquired from the phantoms.
Human studies were performed with six healthy volunteers, who provided written informed consent to participate. Imaging was performed on a Philips Achieva 3T MRI scanner using a 20cm diameter 19F surface coil (PulseTeq Ltd., UK) placed centrally on their upper back. All participants were instructed to perform 3 deep breaths of PFP/O2, followed by a 30s breath-hold at maximal inhalation. A dynamic unlocalised 19F pulse-acquirefree induction decay (TR = 250ms, θ=90o, number of dynamics=350, scan duration=88s) was acquired over the full breathing manoeuvre on two participants. For all remaining participants, a dynamic 19F 2D spoiled gradient echo sequence was initiated at the start of the breath-hold (θ=50o, TE=1.7ms, TR=4.2ms, bandwidth=500Hz/pixel, FOV=300x300x200mm3, acquisition matrix=24x24, number of dynamics=600, scan duration=60s). In all participants, Gadobutrol was administered intravenously via a MEDRAD power injector (dose = 0.2mmol/kg; rate = 5ml/s), concurrent with the start of breath hold.
Results
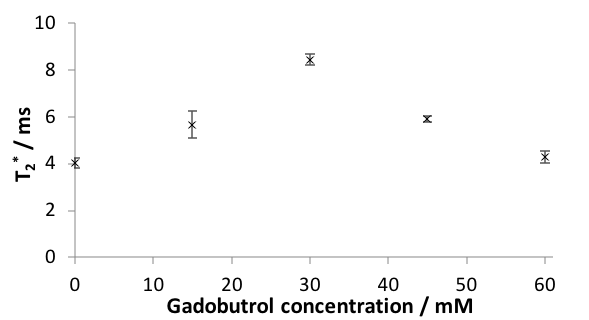
Lung-representative foam phantoms exhibited a PFP T2* of 4.0±0.2ms, markedly shorter than the T2* of pure PFP gas (T2*=12ms), close to that of lung tissue1. Figure 1 shows the change in PFP T2* following the addition of GBCA to the aqueous component of the foam, with maximal T2* values (8.5±0.2ms) achieved at ~30mM, where magnetic susceptibility of aqueous and gas components are matched. The T2* of PFP diminished with increasing Gadobutrol concentrations above 30mM, due to the diverging magnetic susceptibility of gas and aqueous components.
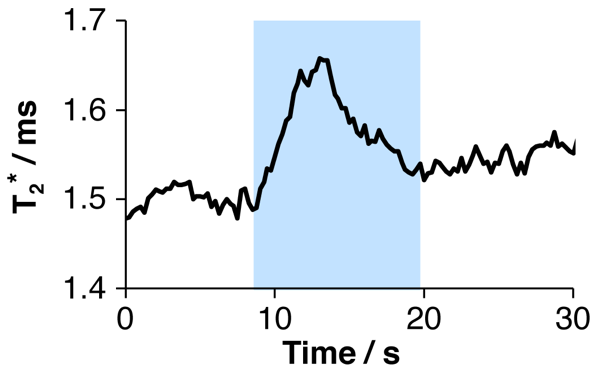
In human studies, dynamic 19F spectroscopy demonstrated a transient rise in PFP T2* following Gadobutrol administration (Figure 2) reflecting the passage of contrast agent through the lungs. Dynamic 2D 19F-MRI scans showed an increase in PFP signal intensity of ~20% shortly after contrast administration (Figure 3).
Discussion
We have demonstrated the feasibility of altering the magnetic susceptibility of alveolar-representative foam phantoms to modify PFP T2* within neighbouring gas components, including determination of the optimum dose of Gadobutrol required to achieve susceptibility matching at alveolar air/water interfaces. This approach offers potential to assess lung microvascular perfusion properties by concurrent administration of inhaled PFP and a paramagnetic contrast agent: the change in PFP T2* reflects a transient reduction in susceptibility differences at alveolar gas-tissue interfaces during first passage of contrast through the pulmonary circulation.Conclusion
To our knowledge, this is the first in man demonstration of this concept. Our approach has implications for assessing combined ventilation/perfusion properties in a short duration radiation-free scan, offering considerable potential for assessing gas exchange in a variety of respiratory pathologies.Acknowledgements
This work was supported by a Medical Research Council Confidence in Concept funding scheme. We are grateful for the contributions of the radiography team at the Newcastle Magnetic Resonance Centre.References
1. Couch, M.J., Ball, I.K., Li, T., et al., Pulmonary ultrashort echo time 19F MR imaging with inhaled fluorinated gas mixtures in healthy volunteers: feasibility. Radiology, 2013; 269(3):903-909.
2. Vignaud, A., Maître, X., Guillot, G., et al., Magnetic susceptibility matching at the air-tissue interface in rat lung by using a superparamagnetic intravascular contrast agent: Influence on transverse relaxation time of hyperpolarized helium‐3. Magn Reson Med, 2005; 54:28-33.
3. Dimitrov, I.E., Insko, E., Rahim, R., Leigh, J.S., Indirect detection of lung perfusion using susceptibility-based hyperpolarized gas imaging. J Magn Reson Imaging, 2005; 21:149-155.
Figures