0008
Improved Pulmonary 129Xe Ventilation Imaging via 3D-Spiral UTE MRI1Cincinnati Children's Hospital Medical Center, Cincinnati, OH, United States, 2Philips, Cincinnati, OH, United States, 3University of Cincinnati, Cincinnati, OH, United States, 4Phoenix Children’s Hospital, Phoenix, AZ, United States, 5Mayo Clinic, Rochester, MN, United States, 6University of Cincinnati Medical Center, Cincinnati, OH, United States
Synopsis
Functional lung imaging via inhaled hyperpolarized 129Xe MRI has been shown to provide sensitive regional maps of ventilation and gas-exchange. Traditionally, ventilation images are acquired via standard Cartesian or less commonly radial sequences. Previously reported results have shown promise for 2D-spiral sequences with increased SNR and/or shorter acquisition lengths. In this study, a 3D-spiral sequence (FLORET) was implemented and compared to Cartesian, radial, and 2D-spiral acquisition techniques. This is the first implementation and comparison of a 3D-spiral UTE technique to acquire hyperpolarized gas images.
Purpose
MRI of inhaled hyperpolarized 129Xe has been shown to characterize regional ventilation in a wide variety of diseases and populations1–10. Ventilation images have most-often been acquired via Cartesian gradient-recalled-echo (GRE) sequences with thick slices (~15mm). The thick slices are implemented to fully acquire the lung volume, limit acquisition time to a breath-hold, and increase SNR. These sequences require few excitations (permitting larger RF flip angles) but suffer from relatively low resolution due to the breath-hold and gradient limitations. Additionally, some groups have begun implementing 3D-radial UTE sequences for more accurate magnetization dynamics and to better quantify ventilation physiology with isotropic resolution4,11–14. However, these sequences are inherently inefficient in k-space sampling, requiring many excitations (forcing lower flip angles for non-renewable magnetization), and may need to be acquired at lower resolution or with undersampling in order acquire within a breath-hold. Comparisons between the GRE and 3D-radial techniques have shown that 3D-radial sequences suffer a factor of ≈2 in SNR losses compared to GRE but better capture physiologically-relevant characteristics (e.g. gravitational dependence)4. In addition, UTE acquisitions allow advanced image corrections and reconstructions4,15–17.
Relative to radial sequences, spiral acquisitions sample k-space more efficiently, overcoming many of the limitations of 3D-radial sequences, while maintaining their advantages (short TE, isotropic resolution, etc.)15,18–20. Previous hyperpolarized gas spiral images have demonstrated dynamic imaging, minimal excitations, and high SNR15,20,21. However, these sequences were 2D, relying on slice selection, and thus resulting in similar limitations to Cartesian ventilation images4. Here, we demonstrate the first use of a 3D-spiral UTE sequence to acquire xenon ventilation images and compare it to standard ventilation sequences.
Methods
The 3D-spiral sequence implemented here (Fermat Looped ORthogonally Encoded Trajectories, FLORET) is based on the Fermat spiral to limit the oversampling of low k values, resulting in higher sampling efficiencies19. Each spiral is projected onto a single cone (between +45° and -45°) with two orthogonal sets of cones required to fully acquire k-space. The spiral was rotated via the golden angle and rapid gradient spoiling was implemented19. 129Xe was hyperpolarized to 30-40% via a Polarean 9820 xenon polarizer; but decayed to 15-25% at time of imaging. Comparative GRE, 3D-radial, 2D-spiral, and FLORET images were acquired in a structured phantom and in healthy adults (N=3). Images were acquired using a home-built xenon coil in less than 16s (maximum breath-hold duration). Flip angles were optimized via , dependent on the number of excitations a 129Xe nucleus would experience22. TR/TE were the shortest possible for each scan (≈2-50ms/0.09-3ms). GRE, 3D-radial, 2D-spiral, and 3D-spiral/FLORET images were acquired using the following comparisons: 1) Highest fully-sampled resolution, 2) Same voxel volume, and 3) equivalent undersampling.
Non-Cartesian acquisitions were gridded and all acquisitions were reconstructed similarly using Graphical Programming Interface23. Following 3D-FFT, UTE images were corrected for off-resonance effects, B1 inhomogeneity, and hyperpolarized signal decay.
Results
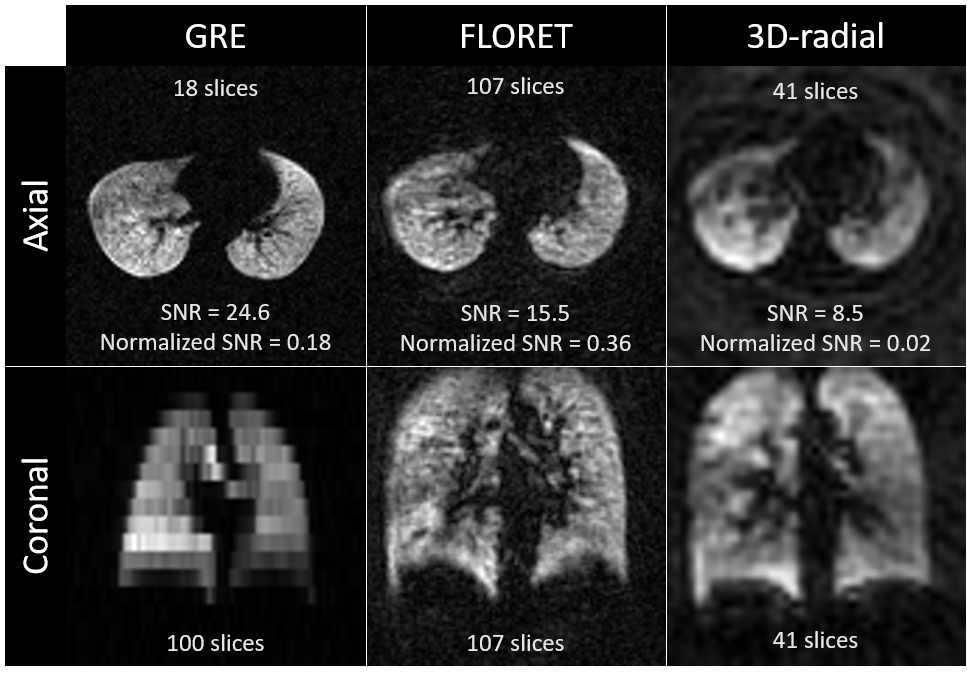
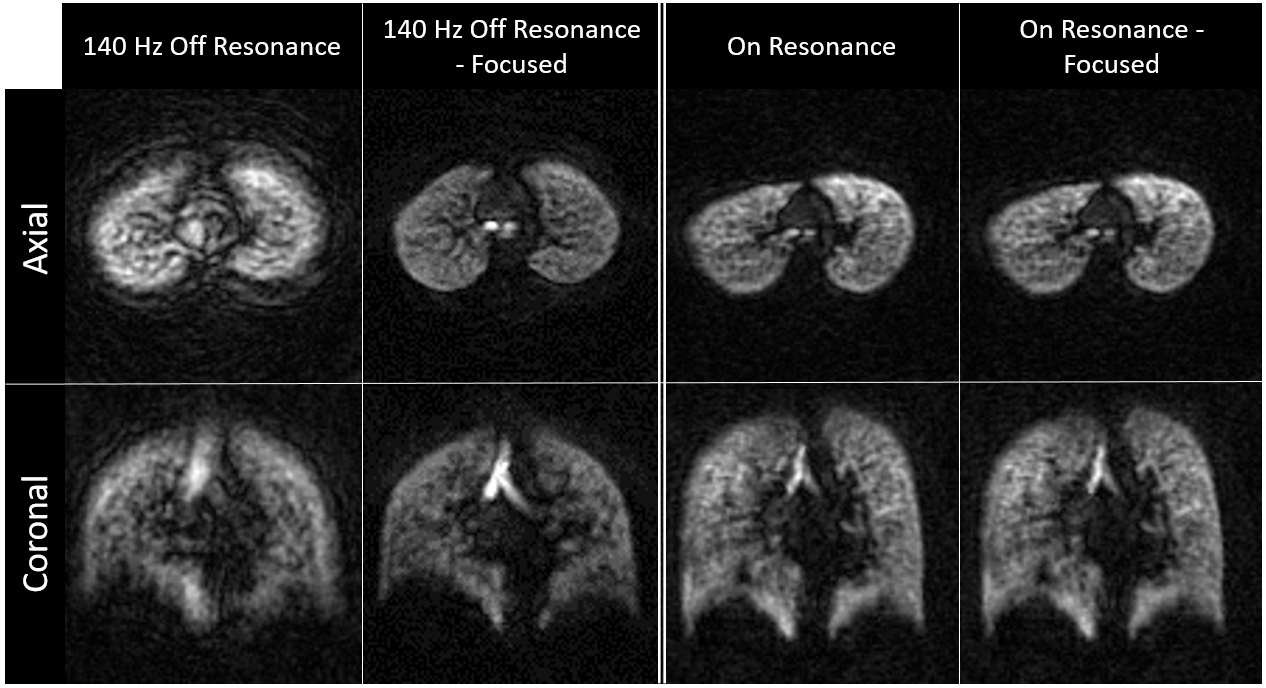
FLORET xenon ventilation imaging allowed a fully sampled image with (3.5mm)3 voxels and a (300mm)3 field of view, to be acquired in 15 seconds, a significant increase in resolution (3.15x smaller voxels) over standard sequences (Figure 1). Additionally, only 262 excitations were necessary (readout duration of 46.3ms), resulting in an SNR-optimized flip angle of 5.5°. However, if the receiver frequency is set imperfectly, the resulting images will exhibit off-resonance blurring/distortion due to the long readout (Figure 2). This can be fixed post-acquisition via off-resonance focusing24.
The standard GRE acquisition had an SNR of 24.6 and an SNR/Vvoxel of 0.18/mm3. 3D-radial images had an SNR of 8.5 and an SNR/Vvoxel of 0.02/mm3. FLORET resulted in an SNR of 15.5 and an SNR/Vvoxel of 0.36/mm3. The reported SNRs are without additional post-processing corrections, which would result in improved image quality for the UTE sequences.
Discussion
FLORET acquired higher resolution xenon ventilation images when compared to traditional GRE and 3D-radial sequences. When accounting for voxel volume, FLORET outperformed both GRE and 3D-radial with respect to SNR. Additionally, FLORET benefits from acquiring k0 in every projection, allowing for future corrections such as B1 inhomogeneity and magnetization decay.Conclusion
Highly-efficient UTE MRI spiral sequences allow for higher resolution, isotropic, fully-sampled xenon ventilation images. FLORET’s fewer excitations allows for higher flip angles and normalized SNR over GRE and 3D-radial images. Sampling k0 each projection permits image corrections and improvements. For a given magnetic moment and breath-hold, 3D-spiral ventilation imaging would permit detection of smaller ventilation defects, smaller changes in ventilation, shorter breath-hold durations, and/or time-resolved ventilation – advantages which are particularly crucial when implementing in pediatrics, where patients’ anatomy is small and breath-hold compliance is lower.
Acknowledgements
The authors thank the following sources for research funding and support: NIH R01 HL131012 and NIH R44 HL123299. Additionally, the authors would like to thank Ashley G. Anderson III PhD (Philips Healthcare) for the ability to implement the off resonance focusing code they developed.References
1. Driehuys B, Martinez-Jimenez S, Cleveland ZI, et al. Chronic obstructive pulmonary disease: safety and tolerability of hyperpolarized 129Xe MR imaging in healthy volunteers and patients. Radiology. 2012;262(1):279-289. doi:10.1148/radiol.11102172.
2. Mugler JP, Altes TA. Hyperpolarized 129Xe MRI of the human lung. J Magn Reson Imaging. 2013;37(2):313-331. doi:10.1002/jmri.23844.
3. Virgincar RS, Cleveland ZI, Sivaram Kaushik S, et al. Quantitative analysis of hyperpolarized 129Xe ventilation imaging in healthy volunteers and subjects with chronic obstructive pulmonary disease. NMR Biomed. 2013;26(4):424-435. doi:10.1002/nbm.2880.
4. He M, Robertson SH, Kaushik SS, et al. Dose and pulse sequence considerations for hyperpolarized129Xe ventilation MRI. Magn Reson Imaging. 2015;33(7):877-885. doi:10.1016/j.mri.2015.04.005.
5. Roos JE, McAdams HP, Kaushik SS, Driehuys B. Hyperpolarized Gas MR Imaging: Technique and Applications. Magn Reson Imaging Clin N Am. 2015;23(2):217-229. doi:10.1016/j.mric.2015.01.003.
6. He M, Driehuys B, Que LG, Huang YCT. Using Hyperpolarized 129Xe MRI to Quantify the Pulmonary Ventilation Distribution. Acad Radiol. 2016;23(12):1521-1531. doi:10.1016/j.acra.2016.07.014. 7. Thomen RP, Walkup LL, Roach DJ, Cleveland ZI, Clancy JP, Woods JC. Hyperpolarized 129Xe for investigation of mild cystic fibrosis lung disease in pediatric patients. J Cyst Fibros. 2016. doi:http://dx.doi.org/10.1016/j.jcf.2016.07.008.
8. Walkup LL, Thomen RP, Akinyi TG, et al. Feasibility, tolerability and safety of pediatric hyperpolarized 129Xe magnetic resonance imaging in healthy volunteers and children with cystic fibrosis. Pediatr Radiol. 2016;46(12):1651-1662. doi:10.1007/s00247-016-3672-1.
9. Ebner L, Kammerman J, Driehuys B, Schiebler ML, Cadman R V., Fain SB. The role of hyperpolarized 129xenon in MR imaging of pulmonary function. Eur J Radiol. 2017;86:343-352. doi:10.1016/j.ejrad.2016.09.015.
10. Svenningsen S, Eddy RL, Lim HF, Cox PG, Nair P, Parraga G. Sputum Eosinophilia and MRI Ventilation Heterogeneity in Severe Asthma. Am J Respir Crit Care Med. 2018;197(7):876-884. doi:10.1164/rccm.201709-1948OC.
11. Kaushik SS, Freeman MS, Cleveland ZI, et al. Probing the regional distribution of pulmonary gas exchange through single-breath gas- and dissolved-phase 129 Xe MR imaging. J Appl Physiol. 2013;115(24):850-860. doi:10.1152/japplphysiol.00092.2013.
12. Qing K, Ruppert K, Jiang Y, et al. Regional Mapping of Gas Uptake by Blood and Tissue in the Human Lung using Hyperpolarized Xenon-129 MRI. J Magn Reson Imaging. 2014;39(2):346-359. doi:10.1002/jmri.24181.Regional.
13. Kaushik SS, Robertson SH, Freeman MS, et al. Single-breath clinical imaging of hyperpolarized 129xe in the airspaces, barrier, and red blood cells using an interleaved 3D radial 1-point Dixon acquisition. Magn Reson Med. 2016;75(4):1434-1443. doi:10.1002/mrm.25675.
14. Wang Z, He M, Bier E, et al. Hyperpolarized 129Xe Gas Transfer MRI: The Transition from 1.5 to 3 Tesla. Magn Reson Med. 2018;0(0):1-10. doi:10.1002/mrm.27377.
15. Salerno M, Altes TA, Brookeman JR, Lange EE De, Mugler JP. Dynamic Spiral MRI of Pulmonary Gas Flow Using Hyperpolarized 3He : Preliminary Studies in Healthy and Diseased Lungs. Magn Reson Med. 2001;46:667-677.
16. De Rochefort L, Maître X, Fodil R, et al. Phase-contrast velocimetry with hyperpolarized 3He for in vitro and in vivo characterization of airflow. Magn Reson Med. 2006;55(6):1318-1325. doi:10.1002/mrm.20899.
17. Niedbalski P, Willmering MM, Robertson SH, et al. Mapping and Correcting Hyperpolarized Magnetization Decay with Radial Keyhole Imaging. Magn Reson Med. 2018;SUBMITTED:11.
18. Pipe JG, Zwart NR, Aboussouan EA, Robison RK, Devaraj A, Johnson KO. A new design and rationale for 3D orthogonally oversampled k-space trajectories. Magn Reson Med. 2011;66(5):1303-1311. doi:10.1002/mrm.22918.
19. Robison RK, Anderson AG, Pipe JG. Three-dimensional ultrashort echo-time imaging using a FLORET trajectory. Magn Reson Med. 2017;78(3):1038-1049. doi:10.1002/mrm.26500.
20. Salerno M, Altes TA, Brookeman JR, De Lange EE, Mugler JP. Rapid hyperpolarized 3He diffusion MRI of healthy and emphysematous human lungs using an optimized interleaved-spiral pulse sequence. J Magn Reson Imaging. 2003;17(5):581-588. doi:10.1002/jmri.10303.
21. Doganay O, Wade T, Hegarty E, McKenzie C, Schulte RF, Santyr GE. Hyperpolarized 129Xe imaging of the rat lung using spiral IDEAL. Magn Reson Med. 2016;76(2):566-576. doi:10.1002/mrm.25911.
22. Miller GW, Altes TA, Brookeman JR, De Lange EE, Mugler JP. Hyperpolarized 3He lung ventilation imaging with B1-inhomogeneity correction in a single breath-hold scan. Magn Reson Mater Physics, Biol Med. 2004;16(5):218-226. doi:10.1007/s10334-003-0028-2.
23. Zwart NR, Pipe JG. Graphical programming interface: A development environment for MRI methods. Magn Reson Med. 2015;74(5):1449-1460. doi:10.1002/mrm.25528.
24. Noll DC, Pauly JM, Meyer CH, Nishimura DG, Macovski A. Deblurring for non‐2D fourier transform magnetic resonance imaging. Magn Reson Med. 1992;25(2):319-333. doi:10.1002/mrm.1910250210.
Figures