0007
Differences Between 3He and 129Xe Ventilation Heterogeneity Explained Using Oscillometry1Robarts Research Institute, London, ON, Canada, 2Department of Medical Biophysics, Western University, London, ON, Canada, 3School of Biomedical Engineering, Dalhousie University, Halifax, NS, Canada, 4Division of Respirology, Department of Medicine, Western University, London, ON, Canada
Synopsis
129Xe MRI ventilation defects were previously shown to be greater and more numerous than 3He MRI ventilation defects in patients with chronic obstructive pulmonary disease (COPD) and asthma, however the underlying biomechanical explanation for these differences has not been determined. Here we evaluated the relationships of 3He and 129Xe MRI ventilation defect percent (VDP) with oscillometry measurements acquired in patients to better understand the lung biomechanical constraints that lead to such differences. 129Xe VDP was significantly related to total respiratory-system resistance whereas 3He was not which may suggest increased sensitivity of 129Xe to resistance throughout the entire airway tree.
Introduction
To date, hyperpolarized noble gas MRI has been dominated by 3He because of its high gyromagnetic ratio and the high polarization levels that can be achieved, which results in excellent image quality with relatively small doses. The increased availability, decreased costs and advances in polarization physics1 have shifted most centres to 129Xe. Compared with 3He, 129Xe ventilation was previously shown to be qualitatively more heterogeneous with larger and a greater number of ventilation abnormalities in both asthma2 and chronic obstructive pulmonary disease (COPD).3,4 In COPD, high resistance to flow within emphysematous lung regions was postulated as a potential determinant for the observed 3He and 129Xe ventilation differences.4 Oscillometry probes lung mechanics related to ventilation heterogeneity by applying multi-frequency pressure oscillations at the mouth to measure respiratory impedance, consisting of respiratory resistance (R) and reactance (X).5 Accordingly, the objective here was to investigate the relationships of 3He and 129Xe MRI with oscillometry to better understand the biomechanical factors that lead to different 3He and 129Xe ventilation heterogeneity.Methods
Participants and Data Acquisition: Participants with asthma and COPD provided written informed consent to ethics-board-approved protocols (NCT02351141, NCT02279329) and underwent MRI and oscillometry after administration of a bronchodilator during a single two-hour visit. 1H, 3He and 129Xe MRI were performed within ten minutes of each other using a whole-body 3.0T Discovery MR750 system (General Electric Healthcare, USA) with broadband imaging capabilities. Subjects were instructed to inhale a gas mixture from a 1.0L Tedlar bag from functional residual capacity and image acquisition was performed under breath-hold conditions. Gas mixtures were 100% N2 for 1H, 25% 3He diluted to 1.0L with N2 and 50% 129Xe diluted to 1.0L with 4He. Anatomical 1H MRI was performed before hyperpolarized gas imaging using the whole-body radiofrequency coil and 1H fast-spoiled, gradient-recalled echo (FGRE) sequence with a partial echo (10s total acquisition time, repetition time (TR)/echo time (TE)/flip angle=4.7ms/1.2ms/30°, field-of-view (FOV)=40x40cm, matrix=128x80, 15-17 slices, 15mm slice thickness, zero gap). The order of 3He and 129Xe acquisition was randomized. 3He static ventilation images were acquired using a linear birdcage transmit/receive chest coil and fast-gradient echo method with a partial echo (11s total acquisition time, TR/TE/flip angle=4.3ms/1.4ms/7°, FOV=40x40cm, matrix=128x80, 15-17 slices, 15mm slice thickness, zero gap). 129Xe static ventilation images were acquired using a quadrature-asymmetric birdcage transmit/receive chest coil6 and 3D FGRE method (14s total acquisition time, TR/TE/flip angle=6.7ms/1.5ms/variable, FOV=40x40cm, matrix=128x128, 15-17 slices, 15mm slice thickness, zero gap). Oscillometry was acquired using the tremoFlo C-100 Airwave Oscillometry System (Thorasys, Canada) to measure total respiratory system resistance at 5Hz (R5), frequency-dependence of resistance as R at 5Hz minus R at 19Hz (R5-19) which reflects small airways resistance, reactance at 5Hz (X5) and reactance area (AX) which is the area under the negative part of the reactance curve.
Data Analysis: 3He and 129Xe static ventilation images were segmented to generate ventilation defect percent (VDP) as previously described.7 VDP was defined as the ventilation defect volume normalized to the thoracic cavity volume. A Wilcoxon signed-rank test was performed to compare 3He and 129Xe VDP. Univariate relationships between MRI VDP and oscillometry measurements were assessed using Spearman correlation coefficients.
Results
We evaluated 26 participants including 23 with COPD (75±8 years, 15M/8F) and 13 with asthma (44±9 years, 4M/9F), all post-bronchodilator inhalation. Figure 1 demonstrates qualitative differences between 3He and 129Xe ventilation heterogeneity for participants with COPD and asthma. 129Xe VDP was significantly greater than 3He VDP for participants with COPD (36±22% vs. 19±14%, p<0.0001) but not for participants with asthma (8±11% vs. 6±7%, p=0.2). Quantitative relationships between MRI VDP and oscillometry measurements are shown in Figure 2. For participants with COPD, 129Xe VDP was significantly correlated with R5, R5-19, X5 and AX, whereas 3He VDP was significantly correlated with R5-19, X5 and AX but not R5. For asthmatics, 129Xe VDP was not significantly correlated with oscillometry measurements while 3He VDP was significantly correlated with X5 only.Discussion
Post-bronchodilator values of 129Xe VDP were significantly greater than 3He VDP for COPD but not asthma, in agreement with previous results.2-4 In participants with COPD, 129Xe VDP was significantly related to R5 whereas 3He was not. R5 reflects the resistance of the entire respiratory system and this may suggest that 129Xe is more sensitive to increased resistance throughout the entire airway tree.4 Investigation of pre-bronchodilator relationships in asthma may be necessary to tease out differences with oscillometry.Conclusions
Oscillometry measurements of lung biomechanics reveal increased sensitivity of 129Xe to total respiratory system resistance which helps explain different sensitivities of 129Xe and 3He in patients with airways disease.Acknowledgements
No acknowledgement found.References
1 Walker, T. G. & Happer, W. Spin-exchange optical pumping of noble-gas nuclei. Reviews of Modern Physics 69, 629 (1997).
2 Svenningsen, S. et al. Hyperpolarized (3) He and (129) Xe MRI: differences in asthma before bronchodilation. Journal of magnetic resonance imaging 38, 1521-1530, doi:10.1002/jmri.24111 (2013).
3 Kirby, M. et al. Hyperpolarized 3He and 129Xe MR imaging in healthy volunteers and patients with chronic obstructive pulmonary disease. Radiology 265, 600-610, doi:10.1148/radiol.12120485 (2012).
4 Kirby, M. et al. Pulmonary ventilation visualized using hyperpolarized helium-3 and xenon-129 magnetic resonance imaging: differences in COPD and relationship to emphysema. Journal of applied physiology 114, 707-715, doi:10.1152/japplphysiol.01206.2012 (2013).
5 Oostveen, E. et al. The forced oscillation technique in clinical practice: methodology, recommendations and future developments. The European respiratory journal 22, 1026-1041 (2003).
6 Farag, A., Wang, J., Ouriadov, A., Parraga, G. & Santyr, G. Proceedings of the 20th Annual Meeting of ISMRM, Melbourne, Australia. 1233.
7 Kirby, M. et al. Hyperpolarized 3He magnetic resonance functional imaging semiautom
Figures
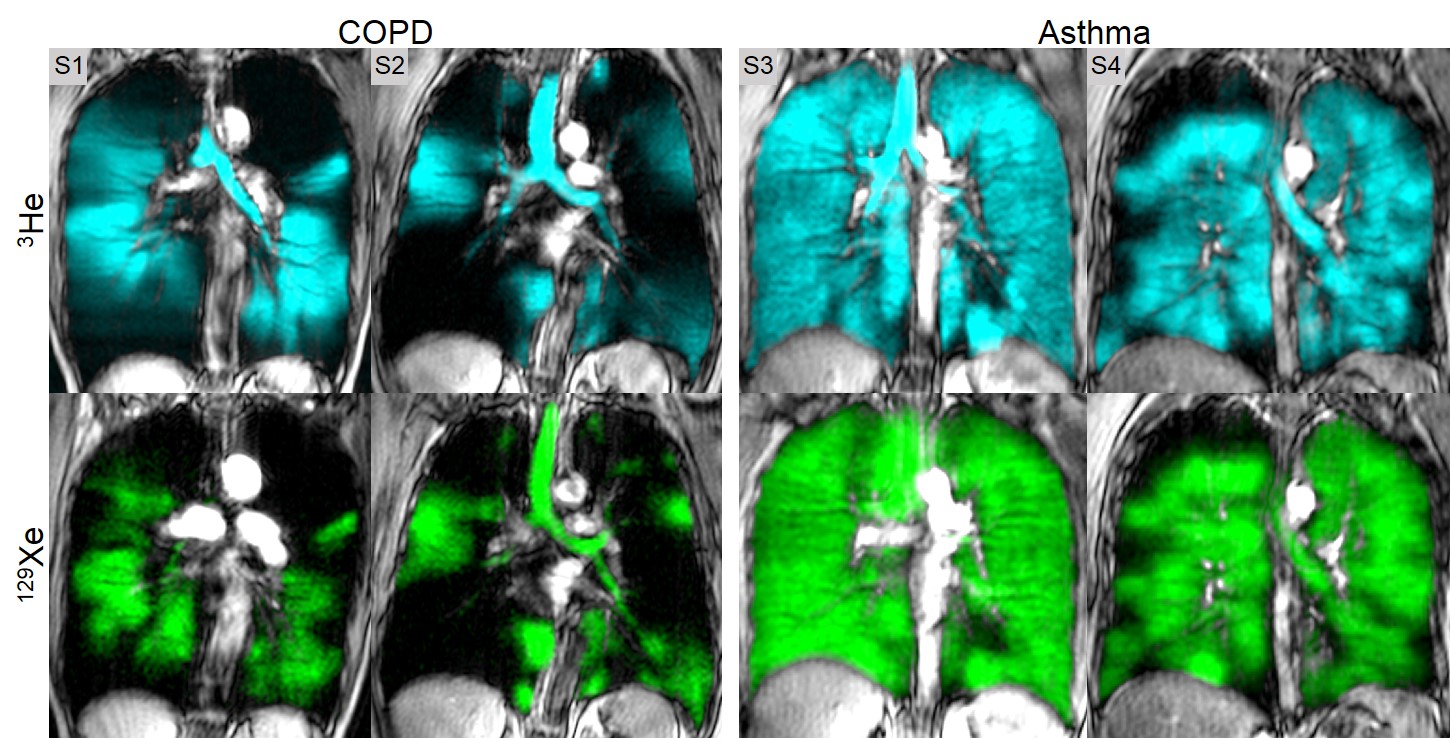
Figure 1. Centre slice 3He and 129Xe static ventilation images for representative participants with COPD and asthma.
Centre slice 3He (cyan) and 129Xe (green) co-registered to anatomical 1H (grey-scale) demonstrates qualitatively more heterogeneous ventilation for participants with COPD but similar ventilation for participants with asthma. S1: VDPHe=26%, VDPXe=42%; S2: VDPHe=45%, VDPXe=64%; S3: VDPHe=2%, VDPXe=2%; S4: VDPHe=13%, VDPXe=15%.
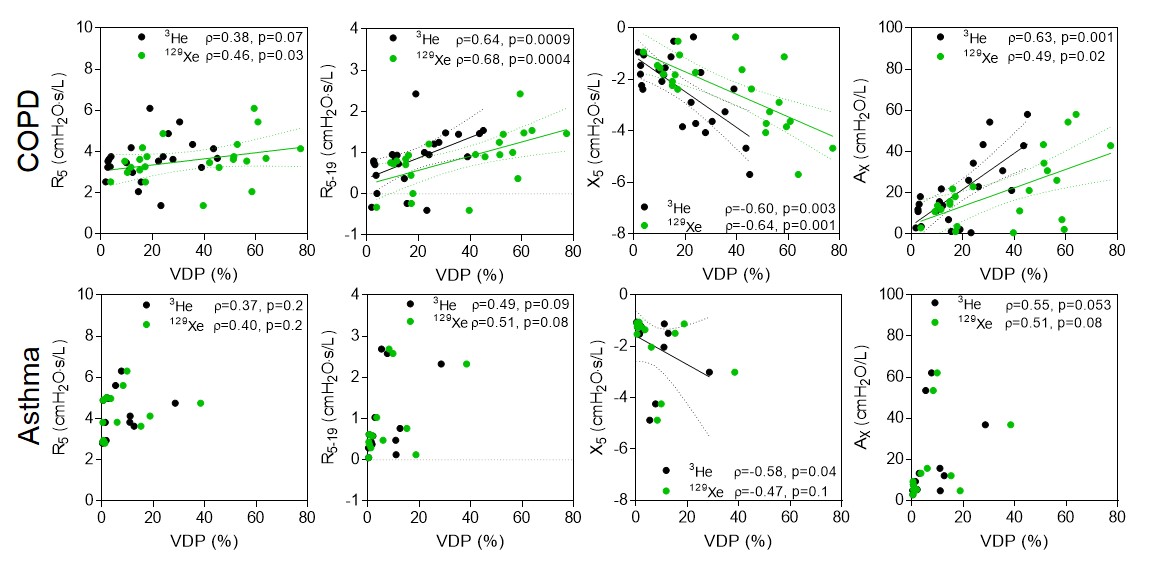
Figure 2. Relationships of 3He and 129Xe MRI ventilation defects with oscillometry.
For participants with COPD, 3He VDP (black circles) was significantly related to R5-19, X5 and AX but not R5, whereas 129Xe VDP (green circles) was significantly related to R5, R5-19, X5 and AX. For participants with asthma, 3He VDP was significantly related to X5 only and 129Xe VDP was not related to any oscillometry measurements.