0006
Comparison of Phase-Resolved Functional Lung (PREFUL) MRI and Hyperpolarized 129Xe MRI in Pediatric Cystic FibrosisMarcus J. Couch1,2, Jonathan H. Rayment3, Robert Grimm4, Andreas Voskrebenzev5,6, Jens Vogel-Claussen5,6, Felix Ratjen1,7, and Giles Santyr1,2
1Translational Medicine Program, The Hospital for Sick Children, Toronto, ON, Canada, 2Department of Medical Biophysics, University of Toronto, Toronto, ON, Canada, 3Division of Respiratory Medicine, British Columbia Children’s Hospital, Vancouver, BC, Canada, 4MR Application Predevelopment, Siemens Healthcare, Erlangen, Germany, 5Diagnostic and Interventional Radiology, Hannover Medical School, Hannover, Germany, 6Biomedical Research in Endstage and Obstructive Lung Disease Hannover (BREATH), Member of the German Center for Lung Research (DZL), Hannover, Germany, 7Division of Respiratory Medicine, The Hospital for Sick Children, Toronto, ON, Canada
Synopsis
Hyperpolarized 129Xe MRI provides robust measurements of ventilatory function through the measurement of the ventilation defect percent (VDP). Recent progress in 1H-based free-breathing techniques (phase-resolved functional lung; PREFUL) allows for the calculation of fractional ventilation maps, which can be similarly processed to calculate VDP. While hyperpolarized 129Xe is an established research technique, PREFUL MRI is simple to implement on any MRI scanner and therefore has good potential for use in future clinical trials in cystic fibrosis (CF). In this study, VDP measurements performed using hyperpolarized 129Xe and PREFUL MRI were compared and correlated with pulmonary function tests in pediatric CF.
Introduction
Free-breathing 1H-based functional lung imaging techniques, such as Fourier Decomposition (FD), provide maps related to ventilation and perfusion.1 Additional post-processing steps can be applied to calculate fractional ventilation (FV) from the free-breathing 1H images using a modified FD reconstruction2 or Phase-Resolved Functional Lung (PREFUL) MRI.3 Hyperpolarized (HP) 129Xe MRI is an established lung imaging technique that is feasible in children with cystic fibrosis (CF)4, and measurements of the ventilation defect percent (VDP), defined as the fraction of unventilated lung, can provide a more sensitive indicator of mild lung disease than spirometric indices, such as the forced expiratory volume in one second (FEV1).5 HP 129Xe VDP is strongly correlated with the lung clearance index (LCI), a measure of ventilation heterogeneity derived from nitrogen multiple breath washout (MBW).6-8 Since HP 129Xe MRI is not widely available, 1H-based functional lung imaging approaches are desirable; however, the application of PREFUL MRI in pediatric CF has been limited to date. The purpose of this study was to compare PREFUL and HP 129Xe MRI and correlate both techniques to LCI and FEV1 in pediatric CF.Methods
24 pediatric participants were recruited (mean age 13±3 years), including 8 healthy controls, 5 with stable well-controlled CF, and 11 CF patients undergoing a pulmonary exacerbation (PEx) at the time of imaging. 9 of the PEx participants returned for a second imaging visit after 2 weeks of treatment. Standard pulmonary function tests were performed, as well as N2 MBW (Exhalyzer D®, EcoMedics AG) to measure LCI (2.5% threshold). Imaging was performed at 3T (MAGNETOM Prisma, Siemens Healthcare) using a flexible 129Xe vest coil (Clinical MR Solutions) and previously described methods.9 Table 1 summarizes the GRE acquisition parameters for the HP 129Xe breath-hold and accompanying breath-hold of N2 for 1H imaging at the same lung volume. Functional 1H MRI was performed by repeating a single central coronal slice TurboFLASH acquisition at a sampling rate of ~3.6 frames per second (Table 1). PREFUL FV maps were calculated using prototype software (MR Lung, Siemens Healthcare)3, and VDP was calculated for both PREFUL and HP 129Xe MRI and using k-means segmentation.9,10Results
Figure 1 shows a comparison of PREFUL FV maps and HP 129Xe MRI acquired in a representative healthy participant and two CF patients. The HP 129Xe VDP represents a whole lung measurement, and the slice most closely matching the location of the FV map is shown. The healthy and stable CF participants had a low VDP as measured by either PREFUL or HP 129Xe. The CF participant undergoing a PEx had substantial ventilation defects in both the PREFUL and HP 129Xe maps, and these defects improved following treatment. Figure 2 shows that the VDP measurements from both techniques are correlated with one another. Figure 3 shows moderate and significant correlations for both VDP calculation methods compared to LCI. Figure 4 shows similar moderate and significant correlations for both methods compared to FEV1. For the PEx participants that returned for a second visit after treatment, there was a statistically significant difference in HP 129Xe VDP and FEV1, but not for PREFUL VDP and LCI (p = 0.020, 0.008, 0.098, and 0.074 from Wilcoxon matched-pairs tests, respectively).Discussion
This study demonstrates a correlation between PREFUL and HP 129Xe VDP in pediatric CF, which qualitatively agrees with similar VDP measurements previously performed using HP 3He and FD MRI in adults with chronic obstructive pulmonary disease.11 The differences in defect regions captured in the segmented maps reflect the complementary nature of the two imaging approaches. The good correlation between VDP and LCI for both techniques suggests that imaging provides a sensitive indicator of ventilation heterogeneity, which is especially important in early CF lung disease where FEV1 often appears normal. Previous work in stable CF has shown a stronger correlation between VDP and LCI6; however, this work includes a broader spectrum of CF lung disease (i.e. PEx). For the whole PEx group, PREFUL VDP was unable to detect significant functional changes following treatment for a PEx, which may point to the need for further image quality optimization. On the other hand, the single-slice nature of the PREFUL acquisition does not necessarily capture regions of the lung that are most affected by the treatment.Conclusions
HP 129Xe and PREFUL MRI are able to provide measures of VDP that are correlated with pulmonary function tests in pediatric CF. PREFUL MRI has a potentially broader applicability in the clinic, since it can be performed on any MRI scanner without inhaled contrast gases, which may be advantageous for young CF patients.Acknowledgements
The authors would like to thank the following individuals for their help with data collection: Yonni Friedlander, Raymond Hu, Nikhil Kanhere, Krzysztof Kowalik, Andras Lindenmaier, Tammy Rayner, Laura Seed, Ravi Seethamraju, Elaine Stirrat, Ruth Weiss, David Wilson, and Brandon Zanette. We would also like to thank the following sources of funding: The Hospital for Sick Children (Catalyst Grant from the Cystic Fibrosis Centre), Natural Sciences and Engineering Research Council of Canada (NSERC) Discovery grant (RGPIN 217015-2013), Canadian Institutes of Health Research (CIHR) operating and project grants (MOP 123431, PJT 153099). MJC was funded by a Research Training Competition (Restracomp) Fellowship from the Hospital for Sick Children and a Mitacs Elevate Postdoctoral Fellowship.References
- Bauman G, Puderbach M, Deimling M, Jellus V, Chefd'hotel C, Dinkel J, Hintze C, Kauczor HU, Schad LR. Non-contrast-enhanced perfusion and ventilation assessment of the human lung by means of fourier decomposition in proton MRI. Magn Reson Med 2009;62(3):656-664.
- Capaldi DPI, Eddy RL, Svenningsen S, Guo F, Baxter JSH, McLeod AJ, Nair P, McCormack DG, Parraga G, Canadian Respiratory Research N. Free-breathing Pulmonary MR Imaging to Quantify Regional Ventilation. Radiology 2018;287(2):693-704.
- Voskrebenzev A, Gutberlet M, Klimes F, Kaireit TF, Schonfeld C, Rotarmel A, Wacker F, Vogel-Claussen J. Feasibility of quantitative regional ventilation and perfusion mapping with phase-resolved functional lung (PREFUL) MRI in healthy volunteers and COPD, CTEPH, and CF patients. Magn Reson Med 2018;79(4):2306-2314.
- Walkup LL, Thomen RP, Akinyi TG, Watters E, Ruppert K, Clancy JP, Woods JC, Cleveland ZI. Feasibility, tolerability and safety of pediatric hyperpolarized 129Xe magnetic resonance imaging in healthy volunteers and children with cystic fibrosis. Pediatr Radiol 2016;46(12):1651-1662.
- Thomen RP, Walkup LL, Roach DJ, Cleveland ZI, Clancy JP, Woods JC. Hyperpolarized 129Xe for investigation of mild cystic fibrosis lung disease in pediatric patients. J Cyst Fibros 2017;16(2):275-282.
- Kanhere N, Couch MJ, Kowalik K, Zanette B, Rayment JH, Manson D, Subbarao P, Ratjen F, Santyr G. Correlation of Lung Clearance Index with Hyperpolarized 129Xe Magnetic Resonance Imaging in Pediatric Subjects with Cystic Fibrosis. Am J Respir Crit Care Med 2017;196(8):1073-1075.
- Walkup LL, Thomen RP, Bell E, Decker B, Cleveland Z, Clancy JP, Woods JC. Quantification of regional ventilation heterogeneity of early cystic fibrosis lung disease via 129xe magnetic resonance imaging: comparison with PFT and LCI. Pediatr Pulmonol 2016;51(S45):351.
- Marshall H, Horsley A, Taylor CJ, Smith L, Hughes D, Horn FC, Swift AJ, Parra-Robles J, Hughes PJ, Norquay G, Stewart NJ, Collier GJ, Teare D, Cunningham S, Aldag I, Wild JM. Detection of early subclinical lung disease in children with cystic fibrosis by lung ventilation imaging with hyperpolarised gas MRI. Thorax 2017;72(8):760-762.
- Santyr G, Kanhere K, Morgado F, Rayment JH, Ratjen F, Couch MJ. Hyperpolarized Gas Magnetic Resonance Imaging of Pediatric Cystic Fibrosis Lung Disease. Acad Radiol 2018;DOI: 10.1016/j.acra.2018.04.024.
- Kirby M, Heydarian M, Svenningsen S, Wheatley A, McCormack DG, Etemad-Rezai R, Parraga G. Hyperpolarized 3He magnetic resonance functional imaging semiautomated segmentation. Acad Radiol 2012;19(2):141-152.
- Capaldi DP, Sheikh K, Guo F, Svenningsen S, Etemad-Rezai R, Coxson HO, Leipsic JA, McCormack DG, Parraga G. Free-breathing Pulmonary (1)H and Hyperpolarized (3)He MRI: Comparison in COPD and Bronchiectasis. Acad Radiol 2015;22(3):320-329.
Figures
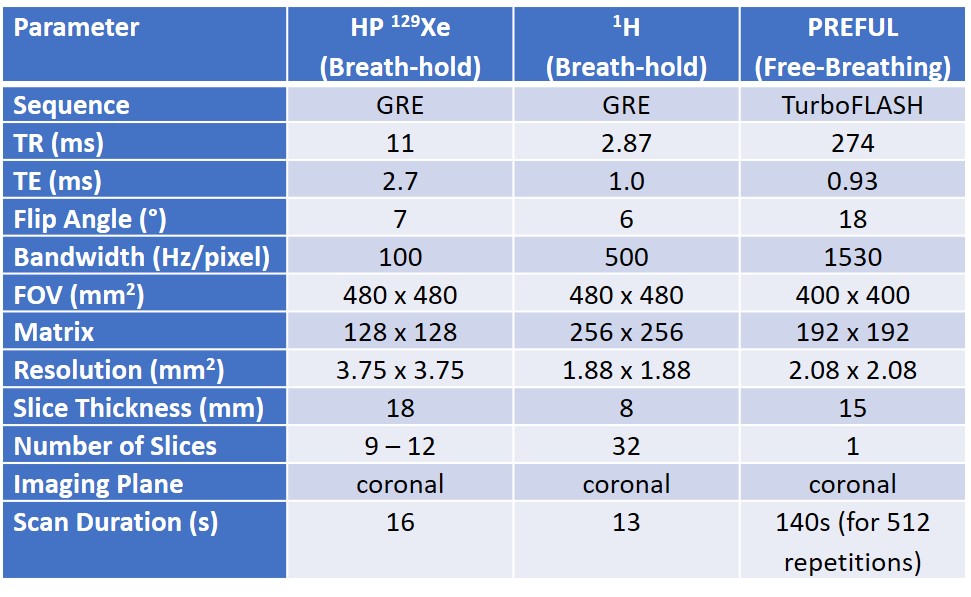
Table 1: Summary of HP 129Xe
and 1H MRI acquisition parameters.

Figure 1: Representative images acquired in (a) a
healthy participant, (b) a stable CF participant, (c) a CF participant
undergoing a pulmonary exacerbation (PEx), and (d) the same PEx participant
after 2 weeks of treatment. From left to right, the images show (i) an overlay
of the 1H TurboFLASH acquisition and the processed PREFUL FV map,
(ii) the segmented FV map showing ventilated areas in green and defect areas in
purple, (iii) an overlay of the 1H GRE and HP 129Xe GRE
acquisitions, and (iv) the segmented 129Xe image showing ventilated
areas in green and defect areas in purple.

Figure 2: Correlation between VDP measurements
performed using PREFUL and HP 129Xe MRI. Overall, there was a
moderate positive and significant correlation, and the spread of the data
points may be due to the single-slice nature of the PREFUL acquisition.
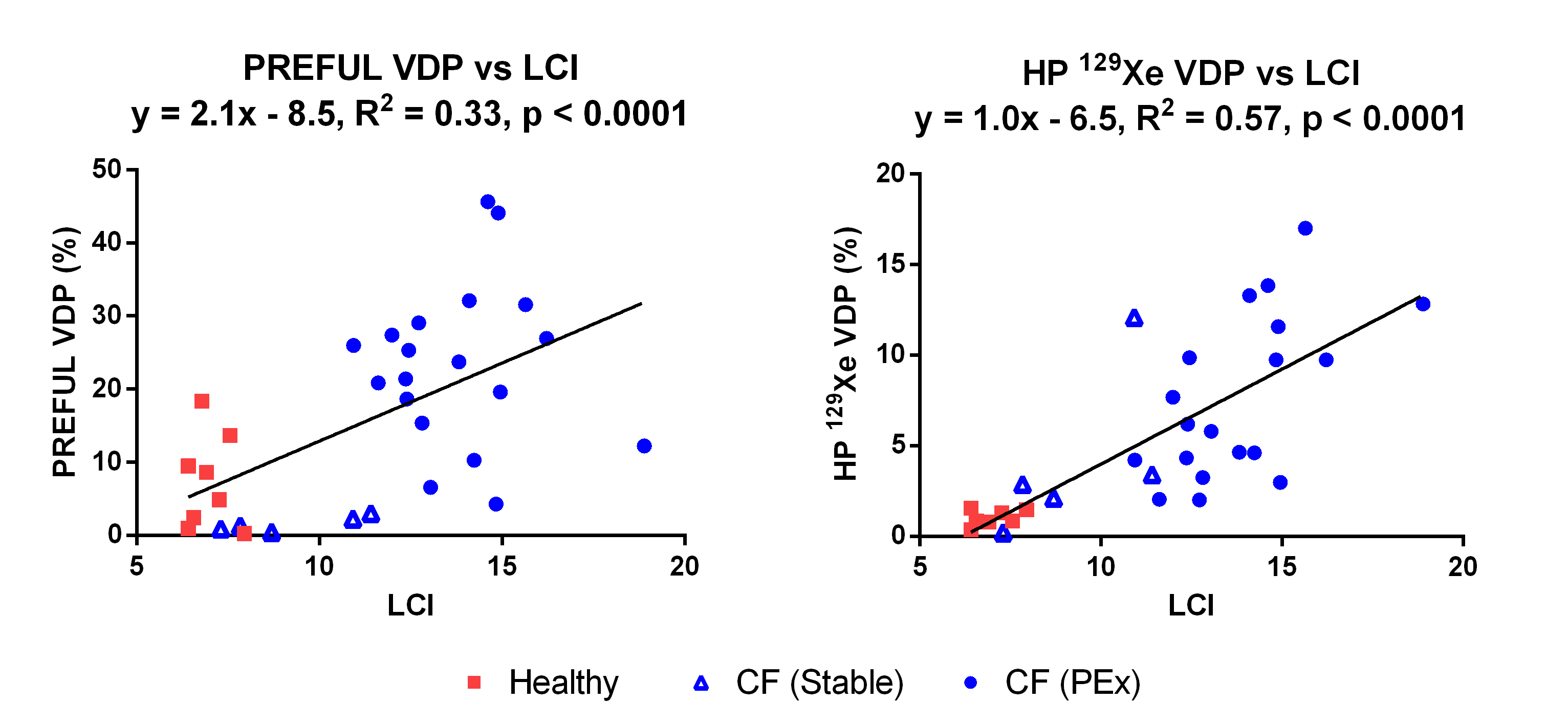
Figure 3: Correlation between VDP and LCI for
measurements performed using (left) PREFUL MRI and (right) HP 129Xe
MRI. In both cases, there was a moderate positive and significant correlation between
VDP and LCI.

Figure 4: Correlation between VDP and FEV1
(as a percentage of the predicted value) for measurements performed using
(left) PREFUL MRI and (right) HP 129Xe MRI. In both cases, there was
a moderate negative and significant correlation between VDP and FEV1.