0003
Improved lung imaging and oxygen enhancement at 0.55T1National Heart, Lung, and Blood Institute, National Institutes of Health, Bethesda, MD, United States
Synopsis
Signal dephasing at high field and low proton density, has limited the use of MRI for lung imaging. We revisit the problem, using a low field (0.55T) scanner which, due to low magnetic susceptibility, improves the signal at air-tissue boundaries like lung. Moreover, because oxygen has increased r1 relaxativity at low field, oxygen inhalation can be used to significantly increase lung signal at 0.55T. Combined, these advantages makes lung MRI lucrative at low field. In this abstract we demonstrate oxygen-enhanced lung MRI at 0.55T in healthy volunteers and Lymphangioleiomyomatosis (LAM) patients.
Introduction
Lung MRI has traditionally been hampered by signal dephasing caused by local susceptibility gradients and low proton density [1]. Low field MRI offers a unique opportunity for lung imaging because of two primary advantages. First, lower magnetic field susceptibility enables imaging near air-tissue boundaries and therefore relative lung signal is increased. Moreover, molecular oxygen [2,3] has increased relaxivity, and inhaled oxygen can act as a powerful signal enhancement agent [4] especially at low field.
Here, we demonstrate that a high performance 0.55T MRI can enable improved ventilation imaging and anatomical lung MRI.
Methods
A commercial 1.5T MRI system (MAGNETOM Aera, Siemens Healthcare, Erlangen, Germany) was modified to operate at 0.55T with maintained gradient performance (45 mT/m maximum amplitude and 200 T/m/s slew rate). Oxygen r1 relaxivity was measured in phantoms for 0.55T. In vivo experiments were conducted under a protocol approved by the local Institutional Review Board. We performed oxygen enhanced lung imaging at 0.55T on 5 healthy volunteers and 4 patients with Lymphangioleiomyomatosis (LAM) [5]. A nonrebreather mask was used to deliver oxygen at 15L/min. Images were acquired following >3 minutes of equilibration time.
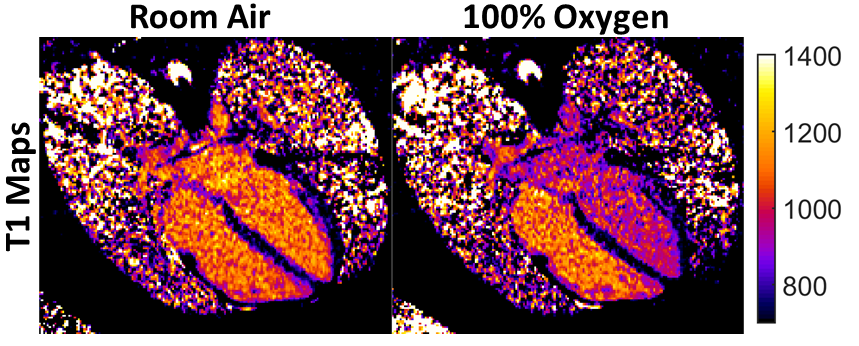
An ultrashort echo time (UTE) stack of spirals prototype sequence [6,7] with T1 weighting was used for 3D anatomical imaging of the lung (TR/TE = 8.54/0.15 ms, flip angle = 20°, slice thickness = 10 mm, FOV = 450 mm x 450 mm, in-plane resolution = 3.5 mm x 3.5 mm, 16 shot spiral design). The data was collected during breadth hold at inspiration for a scan time of 17 seconds. Projection-style lung images were generated from summing the signal of 6 central slices along the slice dimension. T1 was measured in the arterial blood pool and lung during inhalation of room air and 100% oxygen (MOLLI 4(3)3(3)2 scheme with TE = 1.3 ms, TR = 3.2 ms, flip angle = 35°, FOV = 285 mm x 380 mm, matrix = 144 x 256, slice thickness = 8 mm (4 chamber view) or 20 mm (lung)). Comparisons in matched volunteers were also collected at 1.5T.
Results
The improved field homogeneity can be quantified by measurement of the T2* and the T2*:T2 ratio. At 0.55T, T2* is increased to 9ms (from 2ms at 1.5T [8]) and the T2*:T2 ratio is 17% (compared to 5% at 1.5T). In our phantom experiments, molecular oxygen r1 relaxivity at 0.55T was measured to be 4.7e-4 mmHg-1s-1 (vs. 3.1e-4 mmHg-1s-1 at 1.5T). We observed increased baseline lung signal relative to background at low field (Figure 1). The mean UTE signal intensity increase with oxygen inhalation was 18.2± 6.3 % at 0.55T vs 8.6±2.9% at 1.5 T (n = 5 healthy volunteers). T1 was substantially shortened during oxygen inhalation in both the arterial blood pool (Figure 2) and lung at 0.55T (Figure 3 table).
The LAM patients (Figure 4) demonstrated reduced signal enhancement with oxygen inhalation (8.37± 0.26%) due to reduced ventilation, and T1 shortening was limited compared to healthy volunteers (arterial blood: 10.42± 2.3%, lung: 4.89± 2.02%, n = 4 LAM patients).
Discussions
Low field MRI offers unique advantages for lung imaging by virtue of reduced magnetic field susceptibility gradients and increased oxygen relaxivity. MRI has the potential to measure ventilation and may offer advantages over existing nuclear perfusion/ventilation (VQ) scans. The LAM patients imaged here illustrate the promise for the ability to image reduced ventilation.
The contrast provided by inhaled oxygen offers a unique opportunity at low field because of the increased oxygen relaxivity. We observed a substantial T1 decrease in the arterial blood pool during oxygen inhalation because of the dissolved paramagnetic oxygen in the blood, indicating that these oxygen-enhanced methods are promising for imaging oxygenation of the blood and in other tissues. Low-field MRI may act as an avenue for high resolution functional lung imaging [9] which is inaccessible with conventional MRI.
Conclusion
This preliminary investigation of lung MRI illustrates the potential of a low field MRI system for clinical imaging in this region normally suffering from image distortion or signal loss.Acknowledgements
Division of Intramural Research, National Heart, Lung, and Blood Institute (Z1A-HL006213, Z1A-HL006214)References
1. Puderbach, M., Hintze, C., Ley, S., Eichinger, M., Kauczor, H. U., & Biederer, J. (2007). MR imaging of the chest: a practical approach at 1.5 T. European journal of radiology, 64(3), 345-355.
2. Mirhej, M. E. (1965). Proton spin relaxation by paramagnetic molecular oxygen. Canadian Journal of Chemistry, 43(5), 1130-1138.
3. Edelman, R. R., Hatabu, H., Tadamura, E., Li, W., & Prasad, P. V. (1996). Noninvasive assessment of regional ventilation in the human lung using oxygen–enhanced magnetic resonance imaging. Nature medicine, 2(11), 1236.
4. Dietrich, O., Gaass, T., & Reiser, M. F. (2017). T1 relaxation time constants, influence of oxygen, and the oxygen transfer function of the human lung at 1.5 T—A meta-analysis. European journal of radiology, 86, 252-260.
5. Johnson, SR, Taveira-DaSilva AM, Moss J. Lymphangioleiomyomatosis. Clin Chest Med. 2016 Sep;37(3):389–403. DOI:10.1016/j. ccm.2016.04.002. PubMed PMID: 27514586
6. Qian, Y., & Boada, F. E. (2008). Acquisition‐weighted stack of spirals for fast high‐resolution three‐dimensional ultra‐short echo time MR imaging. Magnetic resonance in medicine, 60(1), 135-145.
7. Mugler III, J. P., Fielden, W. S., Meyer, H. C., Altes, A. T., Miller, G. W., & Stemmer, A. (2015). Breath-hold UTE Lung Imaging using a Stack-of-Spirals Acquisition. In Proc Intl Soc Mag Reson Med.
8. Wild, J. M., Marshall, H., Bock, M., Schad, L. R., Jakob, P. M., Puderbach, M., ... & Biederer, J. (2012). MRI of the lung (1/3): methods. Insights into imaging, 3(4), 345-353.
9. Eichinger, M., Optazaite, D. E., Kopp-Schneider, A., Hintze, C., Biederer, J., Niemann, A., ... & Puderbach, M. (2012). Morphologic and functional scoring of cystic fibrosis lung disease using MRI. European journal of radiology, 81(6), 1321-1329.
Figures